Chapter 1. Status of Knowledge, Practice, and Perspectives
Although many older adults (people 65 years and older) experience the benefits of improved oral health—more are retaining their natural teeth and are enjoying a better quality of life as a result—substantial challenges remain for some. Older Americans often face significant obstacles to adequate oral health, including persistent inequities in oral health and difficulties in accessing oral care. The cumulative effects of risk factors associated with poor health, and the potential loss of employer-provided dental insurance benefits for some older adults transitioning into retirement, can adversely affect oral health.
The U.S. population 65 years and older is growing rapidly. Today, 1 in 6 Americans, or 54.1 million, is more than 65 years old (U.S. Census Bureau 2019). By 2030, 1 in 5 Americans—about 70 million people—will be older than 65, increasing to 98.2 million by 2060 (Colby and Ortman 2015). The older adult population in the United States will be one of the most diverse ever in terms of race/ethnicity, socioeconomic status, health, and functional status (Mather et al. 2015). With a graying population and increasing expectations for good oral health–related quality of life, older Americans are seeking dental care in higher numbers than before. Although “progress in prevention and treatment of caries and periodontal diseases has been translated to better oral health and improved tooth retention in the adult population” (Tonetti et al. 2017, p. S135), older adults remain at risk for many oral diseases, including tooth decay, dental root decay, gum disease, and oral cancer. Xerostomia and dry mouth affect a greater percentage of older adults than younger adults and are often side effects of many medications.
About 80% of older Americans live with at least one chronic disease, and nearly 70% have at least two chronic diseases (National Council on Aging 2021). As these diseases progress, physical and neurobiological changes become more common and can lead to disability. The Centers for Disease Control and Prevention reports that 40% of people older than 65 report a physical or cognitive disability (Centers for Disease Control and Prevention 2018a). These disabilities affect the capacity to maintain good oral self-care and negatively impact accessibility and affordability of oral health care (Okoro et al. 2018).
Many baby boomers (individuals born between 1946 and 1964) will keep their teeth longer than any generation before, yet they continue to experience a preventable decline in oral health. As with younger age groups in the United States, older adults experience socioeconomic inequities in tooth loss, untreated decay, periodontal disease, oral cancer, and other oral diseases and conditions. Better access to oral health care improves health outcomes by detecting oral conditions sooner and identifying preventable risk factors, yet there are obstacles to achieving that access.
Barriers to care are not only economic but also include social disparities experienced by all age groups, as well as ageist discrimination, such as the belief that older adults have few or no teeth and do not require routine dental care. Despite higher expectations than ever before for maintaining one’s own natural teeth, society continues to accept declines in oral health related to aging and to make oral health care an elective, rather than a mandatory, part of overall health care. Medicare, the primary form of health insurance for millions of older Americans, excludes dental benefits except in certain narrow circumstances. In addition, the state-to-state variability of adult dental benefits provided through Medicaid perpetuates discrepant perceptions and expectations for oral health care. Most dental insurance is provided through employers’ optional benefit plans, so those who leave full-time work find it hard to afford dental insurance. These discrepancies between medical and dental coverage contribute to the erroneous perception that oral health care is not essential for older adults. This mistaken belief has made oral health care an elective part of our health care system and places the oral health and general well-being of every older American at risk.
Etiology and Prevalence of Oral Diseases and Conditions
The Global Burden of Disease study recognized severe tooth loss—having fewer than nine teeth—and untreated tooth decay as the dental conditions that most diminish health and quality of life (Marcenes et al. 2013). People with chronic conditions, such as diabetes, heart disease, and rheumatoid arthritis, who tend to be older adults, are at higher risk for these oral conditions (Griffin et al. 2009). Common risk factors such as smoking, poor diet, a reduced capacity to care for one’s teeth and obtain professional dental care, and direct or indirect biological mechanisms—such as low salivary flow caused by medications—may contribute to tooth decay and tooth loss (Griffin et al. 2009). Most national surveillance data on these conditions come from health examination surveys that rarely survey homebound persons or long-term care residents, yet it is known that these vulnerable adults have poorer oral health than their peers who are living more independently (Griffin et al. 2012).
Dental Caries
Tooth decay occurs when tooth enamel or exposed tooth roots are demineralized by acidic bacterial by-products of food and drink. If left untreated, the destructive process of dental caries can cause pain, tooth loss, and infection (see Section 2A, Figure 8) that may spread and lead to serious systemic consequences (Pitts et al. 2017). For more information on what causes caries, see Section 2 of this monograph, which focuses on oral health in children and adolescents.
Today, 96% of all non-edentulous older adults (those with some natural teeth) have experienced tooth decay in their lifetime, with untreated tooth decay present in 1 of 6 (Centers for Disease Control and Prevention 2019). Prevalence of untreated caries varies considerably by race/ethnicity and poverty status (Figure 1). Non-Hispanic Black (29%) and Mexican American (36%) adults aged 65 and older were more than twice as likely to have untreated decay than non-Hispanic White (14%) adults. Older adults living in poverty were at least three times more likely to have untreated tooth decay than their higher-income counterparts (33% vs. 10%). A review of surveys conducted among vulnerable, older adults in nine states found that the percentage of non-edentulous adults with untreated decay ranged from 25–53%, with a median value of 40% (Griffin et al. 2019). In 2015–2016, 29% of adults 75 years and older had dental root surface caries (Griffin et al. 2019).
Figure 1
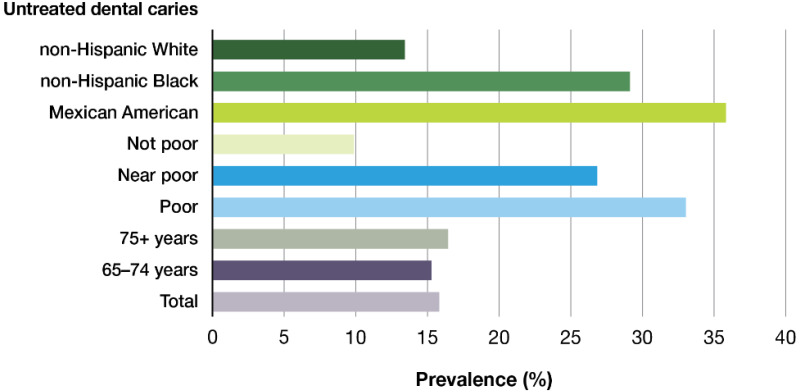
Percentage ot adults ages 65 and older with untreated dental caries in permanent teeth by age group, poverty status, and race/ethnicity: United States, 2011–2016 . Notes: Dental caries experience (DT > 0); FPG = Federal Poverty Guideline: (more…)
About 1 in 6 older Americans experiences root caries (Badr and Sabbah 2020), which is dental caries that affects the area on a tooth surface at or below the demarcation between the coronal and root portions of a tooth (cemento-enamel junction). Older age is associated with a greater prevalence of root caries. However, tobacco use, poor plaque control, xerostomia, lower socioeconomic status, and the inability to afford dental care also are important risk factors (Hayes et al. 2016; Badr and Sabbah 2020; Zhang et al. 2020a).
Periodontal Disease
Periodontitis is a prevalent oral disease in older adults and is typically marked by inflammation of the gums and supporting structures of the teeth, resulting in sore and bleeding gums as well as painful chewing problems. Loss of the supporting structures of the teeth (periodontal ligament and supporting alveolar bone) results from an imbalance in which bacteria residing in the space between the teeth and the gums elicit an inflammatory response, leading to progressive periodontal disease (Hajishengallis 2015). As teeth lose support, mobility and tooth drifting are observed, and periodontal abscesses may occur (see Figure 2, Section 3A), ultimately resulting in tooth loss. As the disease intensifies, bone loss around affected teeth can advance with a worsening infection that can have systemic consequences (Scannapieco and Cantos 2016).
Periodontal disease is associated with chronic diseases such as cardiovascular disease, diabetes mellitus, respiratory disease, and cognitive impairment (Bansal et al. 2013; Teixeira et al. 2017; Cardoso et al. 2018; Liccardo et al. 2019).
The prevalence of any periodontitis (mild, moderate, or severe forms) among older adults is high (Eke et al. 2018). Three in five older adults are affected, with prevalence higher in men, non-Hispanic Blacks and Mexican Americans, and persons with low incomes (Figure 2). Four in five older adults who smoke cigarettes have some form of periodontitis. Among older adults, 9% have severe periodontitis, with prevalence higher among men, non-Hispanic Blacks and Mexican Americans, and persons with low incomes (Figure 3). One in four older adults who are current smokers has severe periodontitis. Periodontitis also varies among states, with prevalence generally higher in the southern half of the United States (Figure 4) (Eke et al. 2016a). This can be attributed to several factors, including the demographics of certain states that have a higher proportion of older adults or racial/ethnic minorities, and that smoking remains more prevalent in some states compared to others (Centers for Disease Control and Prevention 2020a). For more information on periodontitis, see Section 3A of this monograph.
Figure 2
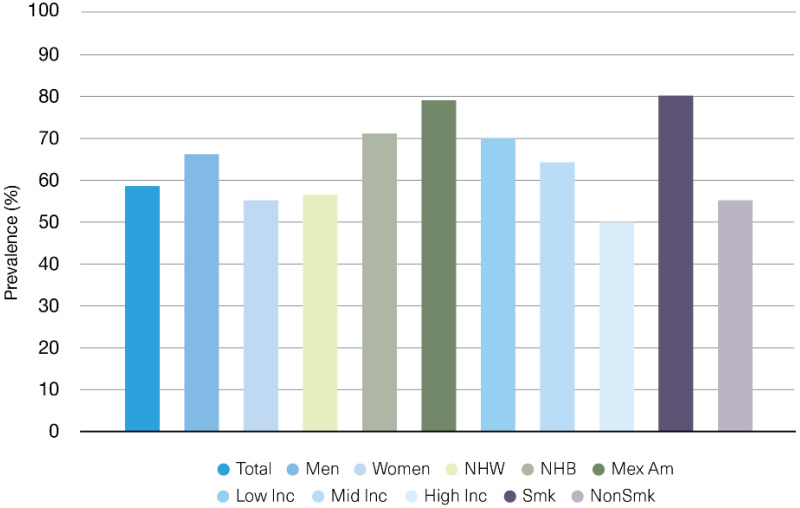
Percentage of adults ages 65 and older with any periodontitis by gender, poverty status, race/ethnicity, and smoking status: United States, 2009–2014. Notes: Any periodontitis includes CDC/AAP mild, moderate, and severe forms. NHW = non-Hispanic (more…)
Figure 3
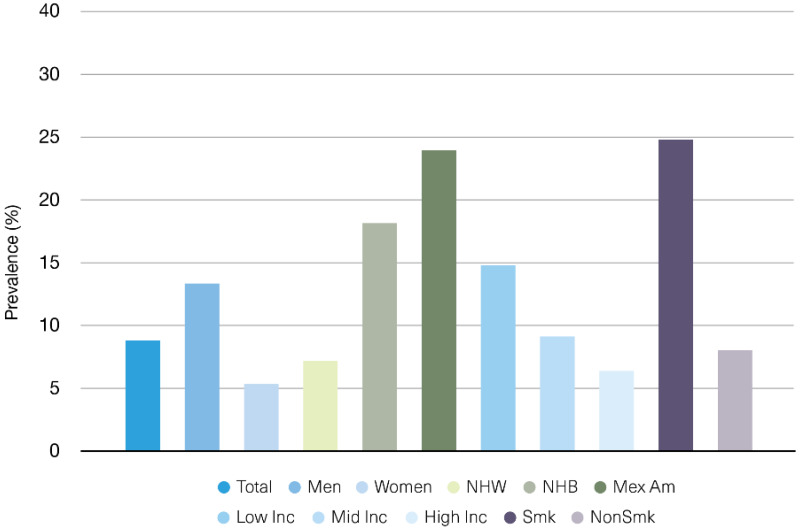
Percentage of adults ages 65 and older with severe periodontitis by gender, poverty status, race/ethnicity, and smoking status: United States, 2009–2014. Notes: Any periodontitis includes CDC/AAP mild, moderate, and severe forms. NHW = non-Hispanic (more…)
Figure 4
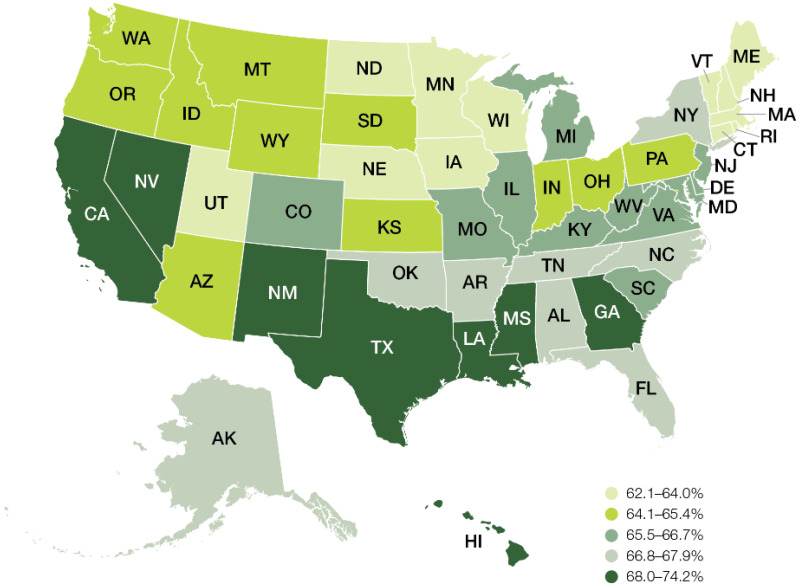
Prevalence of any periodontitis among adults ages 65 and older by state: United States, 2009–2012.
Tooth Loss
The loss of all natural teeth, called edentulism, reduces quality of life because it interferes with the ability to eat, speak, and feel comfortable among other people. Tooth loss affects a person’s ability to consume nutritious food and also can impact how a person eats and socializes with others while consuming food. Edentulism has continued to decline among older adults aged 65 to 74, from about 50% in the 1960s to 13% today (Figure 5) (Dye et al. 2019). Overall, 17% of adults 65 and older are edentulous (Centers for Disease Control and Prevention 2019). Among older adults, persons living in poverty are three times more likely to be edentulous (34%) than those living at 200% or more of the federal poverty guidelines (11%), and non-Hispanic Black older adults are twice as likely (31%) to be edentulous as non-Hispanic White (15%) or Mexican American (17%) older adults.
Figure 5
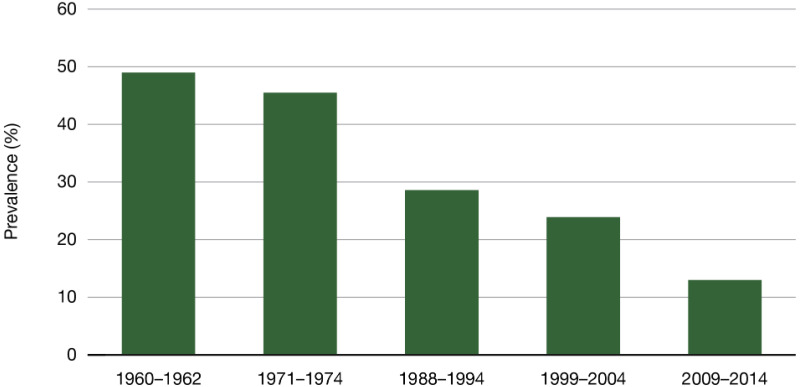
Trend in edentulism among adults ages 65–74: United States, 1960–1962 to 2009–2014. Note: Edentulism is complete loss of all natural permanent teeth.
A recent study from eight states indicated that approximately 32% of vulnerable older adults were edentulous (Griffin et al. 2019). The likelihood that a person has lost all of their teeth also varies by where they live in the United States. Edentulism rates (2018) differ greatly by state for older adults, ranging from approximately 6% (Hawaii) to 26% (West Virginia) (Figure 6) (Centers for Disease Control and Prevention 2018b). In general, edentulism was more common among adults aged 65 and older in specific south-central, midwestern, and northeastern states. Although edentulism rates have substantially improved for older adults, many still experience some tooth loss and are partially edentulous. Overall, older adults have on average 20.7 teeth, and the disparity in tooth retention is substantial between people living in or near poverty and those with family incomes at least twice as high as the federal poverty guidelines (17.6 vs. 22.2 mean teeth) (Centers for Disease Control and Prevention 2019).
Figure 6
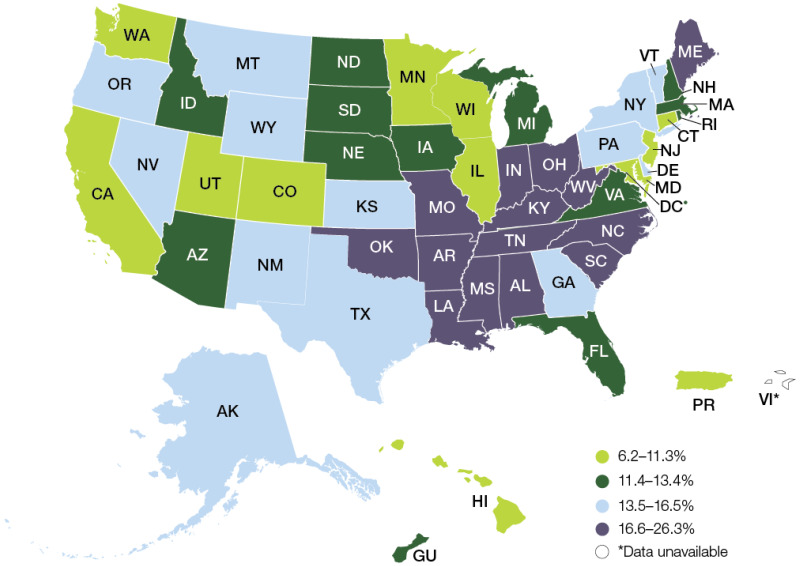
Prevalence of edentulism among adults ages 65 and older by state and territories: United States, 2018. Note: Edentulism is complete loss of all natural permanent teeth.
However, being partially edentulous does not always negatively impact quality of life. Having a functional dentition, that is, having at least 21 natural teeth (Sheiham and Steele 2001; Brennan et al. 2008) or a minimum of 20 teeth, with 9 or 10 pairs of contacting units (Gotfredsen and Walls 2007), is considered necessary for efficient chewing. Three in five adults aged 65 to 74 years have a functional dentition, with substantial disparities observed by poverty status. Only 31% of older adults 65 to 74 living in poverty have a functional dentition, compared to 74% of nonpoor older adults. Differences also exist by race/ethnicity, with prevalence higher in non-Hispanic Whites (78%) and Mexican Americans (70%), and lower in non-Hispanic Blacks (56%).
Among older adults 75 years and older, 46% have a functional dentition, but large differences also exist by poverty status and race/ethnicity. One in five adults 75 years and older living in poverty has a functional dentition, whereas about 1 in 6 non-Hispanic Black or Mexican American adults 75 years and older has a functional dentition (Dye et al. 2019).
The likelihood of an older adult losing some of their natural teeth also varies by where they live in the United States. For adults aged 65 and older who have reported the loss of six or more teeth due to tooth decay or periodontal disease, prevalence varies substantially, from about 22% (Hawaii) to 55% (West Virginia) (Figure 7) (Centers for Disease Control and Prevention 2018b). Similar to edentulism, but with a few exceptions, tooth loss was also more common in many states in the southern regions of the United States.
Figure 7
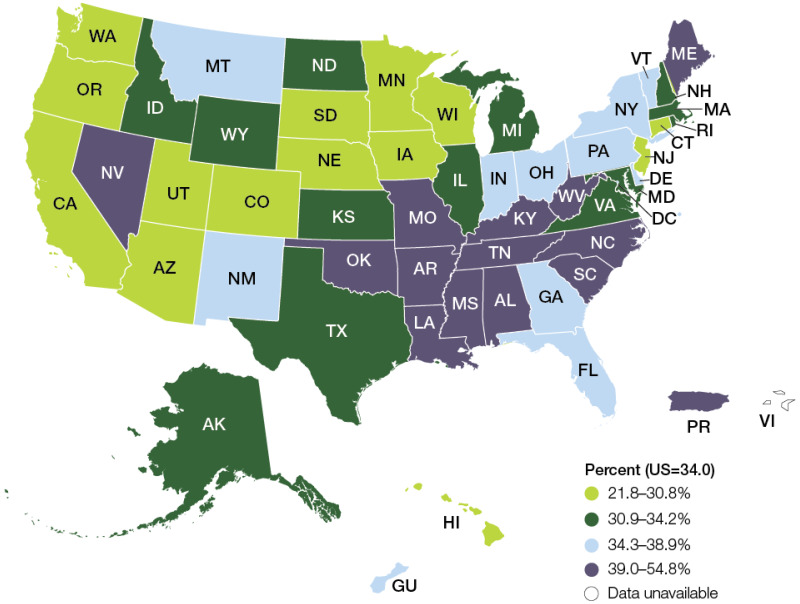
Prevalence of adults ages 65 and older who have lost six or more teeth due to dental diseases by state and territories: United States, 2018.
Having fewer than nine teeth is considered severe tooth loss and can cause major difficulties in eating fruits, vegetables, and meat (Marcenes et al. 2013). Limiting food choices in response to compromised chewing efficiency can result in either weight loss or obesity (Griffin et al. 2012). Extensive tooth loss also detracts from physical appearance and impedes speech, which in turn can restrict social contact and job prospects, inhibit intimacy, lower self-esteem, and impact overall quality of life (U.S. Department of Health and Human Services 2000).
The Global Burden of Disease estimates that U.S. productivity losses attributable to severe tooth loss equaled $32.7 billion in 2015 (Righolt et al. 2018). Nearly one-quarter of adults 65 and older suffered severe tooth loss (Griffin et al. 2019). Prevalence of severe tooth loss was significantly higher among racial/ethnic minorities—46% for non-Hispanic Black and 28% for Mexican American older adults—than among non-Hispanic White adults (22%). Likewise, severe tooth loss was notably higher among lower-income (42%) than higher-income (16%) older adults (Griffin et al. 2019). Recent studies suggest that missing teeth also may be a marker for lifelong, accumulated inflammatory burden of oral disease and may be a risk factor and occur concomitantly with cardiovascular disease (Liljestrand et al. 2015; Lee et al. 2019). Longitudinal studies also have reported associations between the number of missing teeth and cardiovascular disease. Tooth loss is associated with incident mortality resulting from a myocardial infarction (Oluwagbemigun et al. 2015) and is associated with a sevenfold increased risk for mortality from coronary heart disease in persons with fewer than 10 teeth compared to those with more than 25 teeth (Holmlund et al. 2010). National studies have found that adults with diabetes have a higher risk of tooth loss and edentulism than those without diabetes (Patel et al. 2013; Luo et al. 2015). In general, evidence is growing that clearly supports a relationship between increasing tooth loss and adverse health effects in older life.
Oropharyngeal Cancer
Although the increasing prevalence of human papillomavirus (HPV) infection has led to a substantial increase in oropharyngeal cancers among adults aged 40 to 59 years, these cancers remain more prevalent in older adults with a median age at diagnosis of 63 years (National Cancer Institute 2020). Because oropharyngeal cancers are seen more often in older persons than in younger adults (Chi et al. 2015; Tota et al. 2019), these cancers continue to be a public health concern for older adults. The mortality rates for these cancers are higher for older adults (median age of death is 68 years) than for working-age adults (Figure 8) (National Cancer Institute 2020a). Oral cancers can occur anywhere in the oral cavity, while oropharyngeal cancers primarily affect the pharynx, back third of the tongue, soft palate, side and back walls of the throat, and tonsils (see Figure 1 in Section 3A of this monograph). The most common sign is a sore throat or enlarged lymph node (lump or mass in the neck). Table 1 lists the full range of signs and symptoms of oropharyngeal cancers (American Society of Clinical Oncology 2021). See Section 3A for more information on oral cancer and HPV.
Figure 8
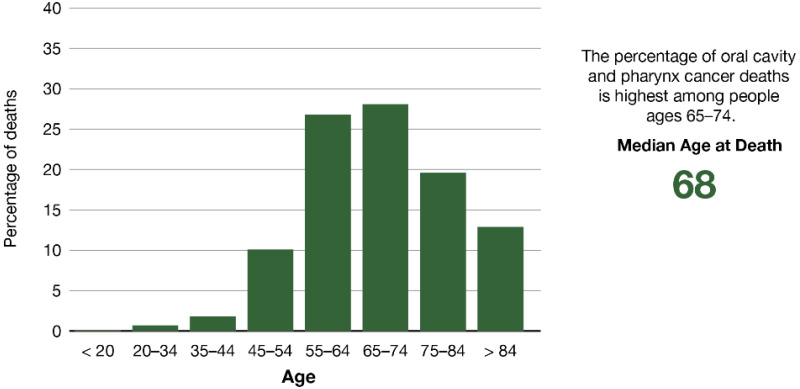
Percentage of deaths by age groups for those diagnosed with oropharyngeal cancer: United States, 2014–2018.
Table 1
Cancer of the oral cavity and pharynx: Symptoms and signs.
Heavy tobacco and alcohol use (defined as two or more packs per day and four or more drinks per day) and the interaction of the two are considered the traditional risk factors for oral cavity and pharyngeal cancers (Blot et al. 1988), particularly squamous cell carcinomas (SSCs). More recently, some subtypes of the human papillomavirus (HPV) also have emerged as a major etiologic factor for this group of cancers. Some studies show that quitting smoking can decrease the risk of these cancers 10 years after cessation, and vaccination against HPV for prevention of cervical cancer also shows great potential for preventing oral and pharyngeal squamous cell carcinomas (Chi et al. 2015). Nearly 9 in 10 oral cancers is SSC, and it is the 11th most common cancer globally (D’Souza and Addepalli 2018). Males are more likely than females to develop oral cancer because of their greater consumption of alcohol and tobacco products (National Institute of Dental and Craniofacial Research 2021). Other implicated risk factors include excess exposure to ultraviolet radiation and cancer of the lip (Samarasinghe et al. 2011). Lip SCC rates declined substantially from 1975 to 2005, but have since remained flat at a rate of 0.6 per 100,000 men and women per year in the U.S.
The median age at diagnosis is 69, and the 5-year relative survival rate is 90.9% (National Cancer Institute 2020b). Globally, rates for cancer of the lip and mouth vary substantially, with rates highest in parts of south-central Asia and Oceania (Miranda-Filho et al. 2019).
Infection with HPV is a major risk factor for oropharyngeal cancers (Chi et al. 2015). The prognosis for older adults with oropharyngeal cancer is mostly dependent on the specific location and extent of the tumor, as well as the presence of regional or distant metastasis (Goldenberg et al. 2014). Five-year relative survival rates for all oral and oropharyngeal cancers range from 73% for localized tumors of the lip to only 12% for metastatic tumors of the oropharynx (Sanabria et al. 2007). In addition, there is some evidence to suggest that being older than 65 years is independently associated with poor prognoses among adults with oropharyngeal cancer (Camilon et al. 2014). The impact of cancer therapy on quality of life among survivors depends on stage at discovery, tumor site, degree of side effects, symptom and treatment management strategies, and the specific organs involved (Valdez and Brennan 2018).
Oral structures in proximity to surgical sites and radiation fields may be affected and compromise the ability to eat, chew, and swallow. They may undergo significant alteration from surgery and radiation therapy, even when not directly affected by cancer (Kent et al. 2015; Choi et al. 2016; Epstein et al. 2018).
The effects on the oral cavity of multiple, potentially aggressive procedures—surgery, radiation, and chemotherapy—may place patients at elevated risk for dental disease. Moreover, oral health may be overlooked during cancer treatment because of lack of insurance or limited medical-dental integration in oncology centers.
Cancer survivorship can mean several different things to many people, but survivorship often means living with cancer beyond treatment. In 2019, there were an estimated 374,000 oral cavity and pharyngeal cancer survivors in the United States. By 2030, that number is expected to grow to nearly 475,000 (American Cancer Society 2019). This projected increase is partly due to the emergence and rapid rise in HPV-related oropharyngeal carcinomas. Disparities in survival exist based on race and ethnicity, with minorities diagnosed at later stages partially due to insurance status (Ragin et al. 2011). Older adults with low education or low income also have worse survival rates (Choi et al. 2016).
Although the American Cancer Society provides clear guidelines on the care needed to minimize risk of some adverse outcomes (Cohen et al. 2016), practitioners and patients face continued challenges, including a lack of predictable protocols to navigate posttreatment issues.
Specific challenges include accessing care for dental disease prevention and speech pathology, which often are not covered by health insurance. Other challenges are the management of the side effects of chemotherapy drugs, intravenous bisphosphonates, and radiation therapy.
Orofacial Pain and Temporomandibular Disorders
Orofacial pain can significantly affect quality of life in older adults. Although it is not known how many older adults experience orofacial pain, some studies suggest that orofacial pain frequently affects older adults with mild cognitive impairment and dementia (Delwel et al. 2017; Delwel et al. 2019). Orofacial pain in older adults can originate inside the mouth from tooth-related or gum infections; or it may originate outside the mouth, such as pain in the jaw joint area, or face and cheeks. Orofacial pain often results from ill-fitting dentures or a microbial infection causing an inflammatory reaction known as denture stomatitis.
Temporomandibular joint and muscle disorders (TMDs) are conditions characterized by pain affecting the temporomandibular jaw joint and the muscles used for chewing in the temporomandibular region (see Figure 6 in Section 3A). TMD can cause functional problems, such as limiting how widely the jaw can open, deviant jaw patterns, and joint sounds (The Advisory Committee of the Temporomandibular Conference 1983). The prevalence of TMD in adults aged 65 years and older is estimated to be 3–5% in the U.S. population (Yadav et al. 2018). Although diagnoses of TMD decline for all people 65 years and older, the highest prevalence for non-Hispanic White women is at 55 years of age, with subsequent decline. Non-Hispanic Black females and males have a lower prevalence of TMD than Whites in younger years. Individuals of lower socioeconomic status have more orofacial pain and pain-related behavioral impacts than individuals of higher socioeconomic status (Riley et al. 2003). Many older adults experience painful conditions such as osteoarthritis and postherpetic neuralgia, which can affect temporomandibular joints (Lautenbacher et al. 2005; Riley et al. 2014). The personal and societal impact of TMD is primarily due to its status as a chronic/recurrent pain condition, and pain is the main reason that patients seek treatment for TMD (Dworkin et al. 1990). Additional information on orofacial pain and TMD disorders is provided in Section 3A.
Salivary Gland Dysfunction and Xerostomia
The term “dry mouth” refers to salivary gland hypofunction (SGH) and xerostomia. SGH means low salivary flow, while xerostomia is the subjective sensation of dry mouth. The exact degree of concordance between these two aspects of dry mouth remains unclear (Villa et al. 2016). Dry mouth is surprisingly common—an estimated 35 million U.S. adults may have xerostomia (Benn et al. 2015). Common causes of xerostomia and SGH include medications, autoimmune disease, systemic diseases, head and neck irradiation, and surgery. A recent systematic review reported the overall prevalence of SGH to be 20% and xerostomia 23%, with prevalence of both conditions highest among older people (Agostini et al. 2018).
Epidemiologic studies in which both salivary gland hyposalivation and xerostomia have been measured are scarce, most likely because of the logistical difficulties of measuring SGH in larger samples. The South Australian Dental Longitudinal Study observed that about 1 in 5 older adults had either xerostomia or SGH, and that the two conditions coincided in only one-sixth of those with either condition—about 6% of the overall sample (Thomson et al. 1999). This was the first empirical evidence to suggest strongly that xerostomia and SGH do not necessarily occur at the same time.
While conditions such as chronic dehydration or anxiety play a part, drugs are by far the most common risk factors for chronic dry mouth. Nearly 9 in 10 (89%) adults aged 65 and older take prescription medicine. More than half (54%) report taking four or more prescription drugs (Kirzinger et al. 2019). However, disentangling the effects of medications on salivary flow and subjective dry mouth is challenging. A particular drug may exert its effect at more than one step in the salivary secretion pathway; and the strength of the effect is determined by dose, duration, metabolism, and the effects of other drugs being taken (Villa et al. 2016).
The drugs most consistently implicated in dry mouth are antidepressants, diuretics, anti-anginals, bronchodilators, and antihistamines. Polypharmacy (the use of multiple drugs) remains a challenge, especially in older adults, and only a few studies have assessed its impact on dry mouth (Johnson et al. 1984; Thomson et al. 2000; Thomson et al. 2006a; Singh and Papas 2014). Chew and colleagues (2008) introduced the concept of anticholinergic burden, in which the greater the number and dosage of these types of common drugs being taken, the greater the likelihood and severity of side effects, such as dry mouth. In addition, many older adults treated with radiation for head and neck cancer experience very severe dry mouth or xerostomia, with many complications, such as rampant cervical and root caries.
The impact of dry mouth is considerable, as shown consistently by epidemiologic studies (Locker 2003; Gerdin et al. 2005; Thomson et al. 2006b; Ikebe et al. 2007; Enoki et al. 2014; Benn et al. 2015). Ikebe and colleagues (2007), for example, observed a strong association between dry mouth and quality of life among older Japanese adults who had xerostomia or SGH, suggesting that both aspects of dry mouth can affect quality of life. Individuals with xerostomia and SGH may have problems with eating, speaking, swallowing, or wearing dentures, and often need to sip liquids while eating. The crucial role of saliva in tasting foods means that there also may be taste alterations, with persons unable to enjoy their food as much as before (Turner and Ship 2007).
Halitosis, burning mouth/tongue, and intolerance of acidic or spicy foods can lead to changes in diet that also can have an adverse effect on nutritional status and quality of life (Atkinson and Wu 1994). Dietary changes also can be induced as a result of difficulty in using dental prostheses, with a lack of saliva in the denture-mucosa interface producing denture sores. Although speech and eating difficulties are perhaps most severe in those who have undergone radiation treatment for head and neck cancer (Turner and Ship 2007), they also are apparent among less severely affected dry mouth sufferers. Amifostine is a medication sometimes provided to relieve dry mouth during head and neck cancer treatment. However, there is insufficient evidence to suggest that amifostine prevents the feeling of dry mouth while receiving radiotherapy to the head and neck (with or without chemotherapy) in the short or medium term following radiation treatment (Riley et al. 2017). There is limited evidence for nonpharmacological interventions, including acupuncture and electrostimulation, for the treatment and relief of dry mouth (Furness et al. 2013).
High-Risk Behaviors Affecting Oral Health in Older Adults
High-risk behaviors are generally less common among older adults than in younger age groups. About 9% of those 65 years and older reported that they were current smokers, and 8% reported excessive alcohol consumption, defined as having five or more drinks in one day at least once in the past year (Han and Palamar 2020). Cannabis use also is on the rise among seniors, increasing from less than 1% in 2006/2007 to 3% in 2015/2016, and more than 4% in 2018. See Section 5 for more information on substance use.
Social Determinants of Health
Social determinants of health (SDoH) are key social and economic factors that influence individual and population health. SDoH concepts described in Healthy People 2030 include the domains of economic stability, health care access and quality, neighborhood and built environment, social/community context, and education access and quality (U.S. Department of Health and Human Services 2020). All of these concepts relate to oral conditions among older adults. For example, access to care, education, and income are strongly related to tooth loss, periodontal diseases, and dental caries. A broader discussion on SDoH is provided in Section 1 of this monograph.
In immigrant communities, oral health risks for older people also are compounded by difficulties in accessing health care and by multiple linguistic, cultural, economic, and social barriers. Acculturation plays a role in oral health status and promotion and can either support or negatively impact oral health. Cultural beliefs can influence both health care choices and service use. For instance, in Asian cultures, friends, neighbors, and family often are consulted before turning to formal services (Esperat et al. 2004). An analysis of studies on the influence of culture on oral health–related beliefs and behaviors of older Chinese immigrants found a common belief that dental caries and tooth loss are inherited conditions and inevitable in old age (Smith et al. 2013). In a study of Dominican, Puerto Rican, and African American older adults, the authors concluded that being sensitive to culture-bound knowledge, beliefs, and behaviors may help to improve health equity for underserved populations (Shedlin et al. 2018). Additional information on acculturation and oral health is discussed in Section 1.
Interrelated Effects of Oral Health with General Health
Older adults’ health status can vary widely, ranging from good health to ill health as the result of comorbid chronic conditions. Some older adults also may have cognitive or functional impairments that require skilled assistance to help with daily activities. Most older adults have at least one chronic health condition, and many have multiple conditions. The more frequently occurring conditions among older adults are hypertension (67% of men 75 years and older and 79% of women 75 years and older), arthritis (54% in 2018 among people 75 years and older), heart disease (28%), any cancer (19% in 2016–2017), and diabetes (28% in 2013–2016) (Administration on Aging 2020).
Oral bacteria and their toxins can spread into the bloodstream through ulcerated or inflamed tissues during chewing, routine oral hygiene, and dental procedures. Plaque and gingival inflammation transiently increase the prevalence of bacteria in the bloodstream following toothbrushing (Lockhart et al. 2009; Matthews 2012). In addition, the presence of oral bacteria or their toxins may induce inflammatory responses, which can prompt insulin resistance (Johnson et al. 2017). Oral bacteria can reach tissues in the lung, heart, gut, placenta, joints, and even the brain. They have been associated with infective endocarditis, and chronic inflammation may contribute to systemic conditions such as cardiovascular disease and diabetes (Aviles-Reyes et al. 2017; Sudhakara et al. 2018; Konkel et al. 2019). Although a large body of literature supporting the interrelationship between oral health (particularly periodontitis) and general health exists, the evidence is insufficient to support or invalidate the notion that treating periodontitis can prevent cardiovascular disease (Berlin-Broner et al. 2017; Sanz et al. 2020).
Common Risk Factor Approach
The Common Risk Factor Approach (CRFA) aims to identify and reduce risk factors common to a number of noncommunicable diseases (World Health Organization 1980; Grabauskas 1987; FDI World Dental Federation 2012), including oral diseases, by taking a comprehensive, integrated public health approach. This approach has the potential to decrease disease severity at a lower cost with greater efficiency and effectiveness than disease-specific approaches. The CRFA addresses upstream factors, such as socioeconomic status and discrimination, and should be used in tandem with downstream factors, such as individual behavior and health status (Bharmal et al. 2015).
Focusing on risk factors shared between chronic systemic and oral diseases/conditions has the potential for broad impact (Watt 2005) when there are population-based interventions. One example is a multi-decade and multi-sector public health approach to tobacco prevention and control that included media campaigns, increased taxation, and policies that established smoke-free environments, resulting in a 67% decline in smoking since 1965 (Janakiram and Dye 2020). A population-level intervention that uses an oral health message to promote overall geriatric health is the long-running public awareness campaign focusing on encouraging people to keep at least 20 teeth by age 80—the 8020 Campaign in Japan (Shinsho 2001; 8020 Promotion Foundation 2021). The general idea is that good oral health and nutrition are linked, and together they facilitate health in older adults. Addressing shared risk factors between oral diseases and noncommunicable diseases provides opportunities to incorporate oral health as an integral part of the messaging and care to positively affect oral and systemic health outcomes (Janakiram and Dye 2020).
Dementia and Cognition
Alzheimer’s disease and related dementias (ADRDs) affect approximately 8.2% of the U.S. older adult population (Dwibedi et al. 2018) and increase in old age; for persons older than 85 years, prevalence reaches more than 40% (Beydoun et al. 2014). Poor oral health in persons with ADRD is well documented, with higher rates of acute and untreated oral diseases and conditions than in older persons without dementia. These oral diseases and conditions include untreated decay and retained tooth roots (Delwel et al. 2017), periodontal inflammation (Leira et al. 2017a; Delwel et al. 2018), ulcerations and infections (Ribeiro et al. 2012; Aragon et al. 2018), and diminished salivary flow, all of which have been linked to both medication use and ADRD (Ship et al. 1990). One report has suggested an association between the periodontal pathogen Porphyromonas gingivalis and the development of ADRD (Dominy et al. 2019).
Memory impairment may increase the risk of these oral diseases and conditions. Older adults with dementia may forget to perform daily oral care and, in the later stages of dementia, forget how to perform oral care. In addition, many caregivers are not comfortable with this task, and oral care may not be prioritized because of the many tasks involved with daily care (Marchini et al. 2019a). It follows that ADRD is a primary risk factor for rapid oral health deterioration (Marchini et al. 2017).
Some studies suggest that the relationship between poor oral health and dementia is bidirectional. A 10-year cohort study found that patients with severe or untreated periodontal disease were more likely to receive a diagnosis of dementia at a later date, and periodontal disease has been hypothesized as a modifiable risk factor for dementia (Noble et al. 2013; Lee et al. 2017a; Lee et al. 2017b). A feedback loop relationship has been hypothesized between poor periodontal status and cognitive status (Yaffe et al. 2004; Petersen and Yamamoto 2005). Patients with mild cognitive impairment are more susceptible to periodontal diseases and edentulism (Petersen and Yamamoto 2005). Related basic science studies looking at the interaction of inflammatory mediators and brain cells suggest that chronic periodontitis can contribute as a peripheral source of pro-inflammatory cytokines entering the nervous system through the blood-brain barrier or through peripheral nerve stimulation (Kamer et al. 2008; Tonsekar et al. 2017), and pro-inflammatory cytokines can stimulate glial cells to produce pathologic protein molecules, which then may cause neuronal damage (McGeer and McGeer 2001; Tonsekar et al. 2017). It is noted that current data on the role of periodontal disease in cognitive functions are inconsistent and warrant future studies that use comprehensive and comparable uniform periodontal measurement methods (Yaffe et al. 2004; Cerutti-Kopplin et al. 2016).
Tooth loss also has been associated with dementia in epidemiologic studies and neurologic testing in animal models (Avivi-Arber et al. 2010; Avivi-Arber et al. 2015; Avivi-Arber et al. 2016). Several studies suggest associations between tooth loss and cognitive function. A systematic review and meta-analysis reported a 22–26% higher risk of cognitive impairment and dementia among people with fewer than 20 teeth (Cerutti-Kopplin et al. 2016). Another meta-analysis of 11 studies showed that tooth loss was associated with a 1.4 times greater rate of developing dementia (Shen et al. 2016). Other studies showed that having more teeth was associated with an almost 50% lower rate of dementia (Oh et al. 2018), and that tooth loss was associated with a 1.34 times greater rate of developing dementia (Chen et al. 2018).
Recent prospective studies have shown similar associations between tooth loss and deficient cognition (Tsakos et al. 2015; Sato et al. 2016; Li et al. 2017; Saito et al. 2018). A longitudinal cohort study in Sweden reported a positive association between tooth loss, periodontal bone loss, and cognitive function (Nilsson et al. 2018). Another study among English older adults showed an association of early-stage cognitive impairment with poor oral health and greater risk of tooth loss (Kang et al. 2019).
Aging can affect oral sensorimotor functions and their control (e.g., swallowing or speaking) (Bakke et al. 1990; Karlsson and Carlsson 1990; Kossioni and Karkazis 1998; Lewis et al. 2013; Lin et al. 2017; Peyron et al. 2017; Avivi-Arber and Sessle 2018). About 1 in 5 older adults is orally disabled because of tooth loss associated with reductions in efficiency of chewing, bite force, altered patterns of mastication and speech, and reduced quality of life (Jacobs 1998; Feine and Carlsson 2003; Trulsson et al. 2012; Cerutti-Kopplin et al. 2016; Avivi-Arber and Sessle 2018). Older adults with such impaired oral sensorimotor functions are more likely to have neurological disorders than those with intact sensorimotor function (Daniels 2006; Onder et al. 2007; Martin 2009; Schimmel et al. 2017).
While oral rehabilitation, such as dental implants, can replace lost teeth and restore oral function, they also produce new changes to compensate for the missing periodontal tissues (Avivi-Arber et al. 2015; Avivi-Arber et al. 2016), and neuroplastic changes occur in the sensorimotor cortex of humans with tooth loss. Oral rehabilitation has been shown to reverse these neuroplastic changes and improve an individual’s ability to eat and chew food (Luraschi et al. 2013; Avivi-Arber and Sessle 2018; Kumar et al. 2018).
Cardiovascular Disease
Coronary heart disease (CHD), a form of cardiovascular disease, is the leading cause of death and morbidity in the United States and around the world (GBD 2013; Causes of Death Collaborators 2015). It has become well accepted that chronic inflammation is a risk factor for CHD. Several studies have also suggested that severe periodontitis promotes elevated levels of systemic mediators of inflammation that are risk factors for cardiovascular disease (Schenkein et al. 2020).
It has been suggested that periodontal disease is an independent risk factor for CHD, increasing risk by 24–35% (Humphrey et al. 2008). Studies also have shown an association between atherosclerosis and periodontitis (Almeida et al. 2018). The number of teeth remaining is significantly associated with fatal and nonfatal myocardial infarction (MI), commonly known as a heart attack. The hypothesized link is that MI is closely associated with low-grade chronic inflammation (Holmlund et al. 2017). Research has yet to confirm, however, that treatment of periodontal disease improves cardiovascular outcomes (Humphrey et al. 2008; Li et al. 2014; Liu et al. 2019). A recent review found that, for patients preparing for cardiovascular surgery, there is consensus on the need for screening and treatment of oral-related infections, but a uniform pre-surgical screening approach has not been established (Cotti et al. 2017). Consequently, the authors concluded that guidance on dental care before cardiovascular surgery is needed. Furthermore, individuals with cardiovascular disease should be made aware of the importance of oral health, undergo an oral health risk assessment, and establish a dental home with regular, routine care. Patients often are willing to learn about oral health after an acute cardiac event, after discharge from the hospital, or during rehabilitation following a cardiac event. Further, patients are receptive to nurses educating, assessing, and referring patients for oral care (Sanchez et al. 2017).
Stroke and Cerebrovascular Disease
Stroke is the third-leading cause of death in the United States; nearly three-fourths of all strokes occur in people older than 65 years (Kelly-Hayes 2010). Stroke also is the leading cause of serious long-term disability in the United States, and can have a devastating impact on oral health. A stroke can be ischemic—the result of blockage of a blood vessel supplying the brain—or hemorrhagic, the result of bleeding into or around the brain.
Recent systematic reviews suggest that periodontal disease is associated with stroke (Leira et al. 2017b; Fagundes et al. 2019). Studies evaluating the oral health of patients following a stroke found that these patients have higher levels of plaque and calculus, more gingival bleeding, more periodontal disease, more decayed teeth, and more missing teeth than controls. The more severe the functional disabilities following a stroke, the worse the oral health (Karolyhazy et al. 2018), and poor oral health following a stroke might be associated with rehabilitation outcomes in hospitalized patients (Gerreth et al. 2021). Nevertheless, the evidence is unclear if improving oral care following a stroke reduces the risk of pneumonia or mortality (Lyons et al. 2018).
Studies suggest that poor oral health care and resulting systemic inflammatory markers are associated with an increased risk of recurrent stroke (Sen et al. 2013). Functional deficits, including hemiplegia, apraxia, hypoalgesia, and hyperesthesia following a stroke, may result in fewer dental visits (Sanossian et al. 2011). Difficulty swallowing following a stroke may affect nutritional status and overall health and cause aspiration of food and oral debris. For patients with poor oral health, the bacterial load in oral debris can lead to aspiration pneumonia (Loeb et al. 1999), which is why oral health care among older adults with comorbidities, including those needing long-term care assistance, is important (Oda et al. 2021).
Diabetes and Glycemic Control
Diabetes, in which the body does not make insulin or does not use it the right way, causes dysfunction of the immune system. Studies show a link between chronic inflammation and the development of type 2 diabetes (Simpson et al. 2015). Several pathways by which oral bacteria could potentially influence the metabolic disturbances associated with diabetes have been proposed (Figure 9).
Figure 9
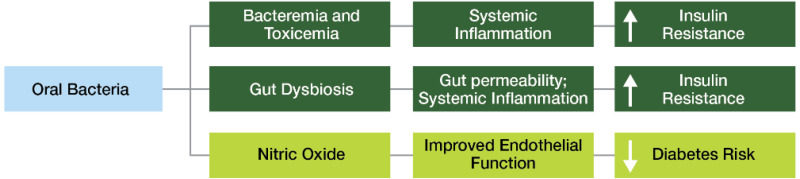
Potential linkage of the oral microbiome to diabetes. Notes: Oral microbiome effects on diabetes: dark green = negative effects, light green = positive effects.
Periodontal disease, an inflammatory condition, has a two-way link with type 2 diabetes. People with diabetes are three times more likely to develop periodontal disease than their healthy counterparts. Diabetes can worsen periodontal disease because it alters the immune response and leads to decreased elimination of associated bacteria.
Conversely, periodontal disease hampers the control of diabetes. Some research suggests that periodontal treatment can decrease systemic inflammation, allowing for better glycemic control (Kudiyirickal and Pappachan 2015), while a clinical trial suggests that periodontal disease treatment in individuals with type 2 diabetes did not improve glycemic control (Engebretson et al. 2013; Geisinger et al. 2016).
Diabetes also is associated with gingivitis, xerostomia, dental caries, oral candidiasis, delayed wound healing, and increased incidence of infection after surgery. In elderly individuals, diabetes is associated with a higher prevalence of root caries, burning mouth syndrome, and candidiasis on the corners of the mouth. In addition, some people with diabetes may be taking medications that cause dry mouth (Kudiyirickal and Pappachan 2015). Older adults with type 2 diabetes and poor metabolic control have poorer health-related quality of life and diminished cognitive functioning (Wandell 2005), compared to those without diabetes. These individuals also are more likely to report poor oral health, dry mouth, and use a dental prosthesis (Azogui-Levy et al. 2018).
Taste impairment and tooth loss, which are more prevalent in older adults, may have a negative impact on diet, thereby affecting an older person’s risk for diabetes or progression of existing diabetes (Muller et al. 2017; Asgary et al. 2018; Guess 2018; Rice Bradley 2018; Burton-Freeman et al. 2019). The impact of these losses on dietary choices and intake are further compounded by coexisting systemic diseases or conditions that impact oral sensory and motor function, such as stroke or Alzheimer’s disease.
Other oral health conditions, such as oral pain, periodontal disease, dental caries, and soft-tissue lesions, also influence nutritional status (Ritchie et al. 2002) and increase the risk for diabetes or compromise diabetes control (Sami et al. 2017). Periodontitis is linked with increased systemic inflammation, dyslipidemia (abnormal lipid levels), and low levels of adiponectin (a protein that regulates glucose and lipids) and can lead to an increased risk of prediabetes and diabetes. Many significant associations between periodontitis and diabetes have been reported in observational studies, suggesting that an important relationship exists between these two diseases. More information on diabetes and oral health in adults is found in Section 3A.
A recent systematic review found significant associations between salivary dysfunction and appetite loss, imbalanced diet, and malnutrition in elderly adults (Munoz-Gonzalez et al. 2018). Xerostomia may lead to inadequate lubrication of the mouth, making it difficult to chew food and swallow. Nutrition therapy is an efficient and cost-effective component of diabetes management (Evert et al. 2019) and is associated with significant improvements in fasting blood sugar, HbA1c, weight, body-mass index, waist circumference, cholesterol, and systolic blood pressure (Razaz et al. 2019).
Diet and Nutrition
Because the mouth is the entryway to the gastrointestinal tract for foods and fluids, any changes in oral soft or hard tissues, including tooth loss, can influence food choices and impact nutrient consumption and nutritional status.
The number and patterns of teeth that best ensure a functional dentition have been defined in a variety of ways, ranging from the number of remaining teeth (Hobdell et al. 2003; Dye et al. 2019) to numbers of occluding (contacting) pairs of tooth surfaces (Sahyoun et al. 2003). The number of natural and prosthetic teeth can affect nutrient intake (carotenes, vitamin C, and folates) of older adults (Ervin and Dye 2012).
Studies show that the risk of malnutrition is greater in adults aged 60 years and older with tooth loss than in those with a complete dentition (Kikutani et al. 2013; McKenna et al. 2014; Toniazzo et al. 2018; Zelig et al. 2018). Kikutani and colleagues (2013) found that community-dwelling, older Japanese adults with inadequate occlusions were at 3.2 times greater risk of malnutrition than those with natural teeth and a functional dentition. People with dentures in the maxilla, mandible, or both were at a 1.7-fold greater risk of malnutrition than those with a functional natural dentition. Older people who were at risk for or had malnutrition had significantly fewer teeth than older adults with no risk of malnutrition (Toniazzo et al. 2018).
Tooth loss—with and without replacement—affects eating behaviors and the overall eating experiences of adults. People with dentures are more likely to engage in certain behaviors such as avoiding raw fruits and vegetables, avoiding eating in public, and eating smaller amounts of foods that require minimal or no biting or chewing (Hyland et al. 2009; Al-Sultani et al. 2019; Zelig et al. 2019). Fear of the dentures making noises, falling out, or causing pain may result in self-imposed limitations on food choices and limit social engagement with others. In contrast, when eating in private, some report positive behaviors, such as peeling and cutting fruits and vegetables, as well as using sauces and broths to moisten tough meats and poultry.
Older men and women who wear dentures consumed fewer servings of fruits and vegetables, especially those rich in carotenes and vitamin C, than did those with teeth (Ervin and Dye 2009). However, it is possible that among the very old, those with well-fitting dentures are able to have more varied nutrient intakes and good dietary quality, compared to those with poorer-fitting dentures or none at all (Marshall et al. 2002). Emerging information is suggesting that tailored dietary advice by dentists offered immediately following delivery of a new set of dentures can improve long-term effects on nutrient intake in edentulous older adults (Kanazawa et al. 2019). Oral health professionals can consider referring patients to a registered dietitian nutritionist for additional information/support.
Osteopenia and Osteoporosis
Research shows that chronic periodontitis is more prevalent and severe in postmenopausal women with osteoporosis than in those with normal bone density. Further, normal levels of vitamin D and use of anti-osteoporosis medication may improve periodontal status in women with osteoporosis (Penoni et al. 2016). Penoni and colleagues (2017), in a systematic review and meta-analysis, verified evidence for the association of periodontal attachment loss with low bone mineral density in postmenopausal women. They found that women with low bone mineral density, compared with those with normal bone mineral density, had greater mean clinical attachment loss (CAL). This indicator reflected a higher mean percentage of sites with CAL equal to or greater than 4 mm, and sites greater than or equal to 6 mm.
Advances in antiresorptive agents (bisphosphonates and denosumab) used to manage osteoporosis have given rise to a concerning oral complication known as medication-related osteonecrosis of the jaws (MRONJ). A systematic review showed that the mean age at onset of MRONJ was 69.7 years, plus or minus 5.2 years; occurrence was more common in females and in the mandible; and alendronate was the most commonly used associated agent. Duration of intake was 50.4, plus or minus 19 months, and 86.7% used the oral route of administration (Aljohani et al. 2017). Longer duration of use seemed to increase the risk of development of MRONJ.
Parkinson’s Disease
Parkinson’s disease is the second most common neurodegenerative disorder, after Alzheimer’s disease, in older people. The gradual degeneration of the brain causes motor, cognitive, and psychiatric symptoms in addition to tremor, rigidity, extreme slowness of movement, impaired balance, and swallowing and speaking difficulties (National Institute on Aging 2017a). Research shows that the body’s inflammatory response affects the progression of Parkinson’s disease, suggesting that chronic inflammation—like that found in periodontal disease—may contribute to the etiology and progression of Parkinson’s disease.
Parkinson’s disease can affect the progression of periodontal disease. Individuals with movement impairment often have trouble performing adequate oral hygiene, leading to poor oral health. In addition, Parkinson’s disease is sometimes associated with cognitive impairment, which can further impair oral hygiene. Research shows that individuals with Parkinson’s disease have more untreated decay, more teeth broken at the gum line, and more bacteria and food debris intraorally than healthy counterparts (van Stiphout et al. 2018). As Parkinson’s disease progresses, individuals may have chewing difficulties (van Stiphout et al. 2018) and worsening periodontal probing depth and clinical attachment loss (Pradeep et al. 2015). The movement difficulties of Parkinson’s disease also make it hard for individuals to travel to a dental office, resulting in fewer dental appointments (Wu et al. 2007).
Osteoarthritis and Rheumatoid Arthritis
Arthritis is a disease of the articular joints and has two main types. Osteoarthritis, the more common form, occurs when cartilage—the tissue that cushions the ends of the bones within joints—breaks down and wears away, causing joint stiffness and pain (National Institute on Aging 2017b). Less common but more destructive, rheumatoid arthritis (RA) is an autoimmune disease that also affects the articular joints. High amounts of bacterial antigens found in the periodontium and gastrointestinal tract may contribute to the etiology of the latter form (Nikitakis et al. 2017). Some studies suggest the periodontal pathogen Porphyromonas gingivalis as a possible trigger for autoimmune disease in some individuals with RA (Kharlamova et al. 2016). Studies also have shown an association between RA and complete tooth loss, as well as periodontal disease (Felton 2016; Bender et al. 2017). Individuals with more severe arthritis note difficulty performing daily oral care and have poorer oral health.
The temporomandibular joint also can be affected and can cause condylar flattening, discomfort, pain, and limited range of motion in severe cases. In addition, individuals may be on high-dose nonsteroidal anti-inflammatory drugs for osteoarthritis, which could increase risk for bleeding following procedures, such as root planing or extractions. Individuals with RA may take corticosteroids or immunosuppressants to manage the disease, increasing the risk of infections, poor healing, and prolonged bleeding, which should be considered in treatment planning and surgical management. In addition, limitations in mobility with advanced disease can make access to care difficult and may limit an individual’s ability to receive treatment owing to discomfort while in the dental chair or the inability to transfer from a wheelchair (Kelsey and Lamster 2008; Chavez et al. 2018).
Sjögren’s Syndrome
Sjögren’s syndrome, the second most common chronic autoimmune disease after rheumatoid arthritis, causes inflammation and fibrosis of the glands that secrete tears and saliva. Although it primarily affects the lacrimal and salivary glands, many other organs and systems within the body, including the respiratory and gastrointestinal systems, also can be affected. Sjögren’s syndrome affects more women than men, generally between 40 and 60 years old. The prevalence for people older than 65 years is much higher than for the general population, varying from five to eight times the prevalence in the younger adult population (0.1–2.7%, depending on criteria used and population studied) (Patel and Shahane 2014). The destruction of the salivary glands by this disease can cause moderate to very severe dry mouth, with reductions in both resting and stimulated salivary flow. Decreased salivary flow, in turn, leads to oral discomfort, difficulty articulating and swallowing, enhanced sensitivity in the oral cavity, and increased fungal and bacterial infections, including tooth decay resulting from loss of the protective components of saliva. The related oral symptoms and disease processes often are compounded in older patients who have other systemic diseases with oral symptoms, or require medications that cause dry mouth (Donaldson et al. 2014).
Medications and Polypharmacy
Specific medications and polypharmacy (the simultaneous use of multiple prescription drugs) affect both salivary flow and the feeling of xerostomia, or dry mouth (Sreebny 1989; Janssens et al. 2017). Janket and colleagues found that taking at least one xerostomic medication was associated with a higher risk of mucosal lesions (Janket et al. 2003; Janket et al. 2007), but a specific association between such medications and other oral diseases, including caries and periodontal disease, has been difficult to establish (Janket et al. 2003; Rindal et al. 2005; Maupome et al. 2006; Syrjala et al. 2011). The issue of polypharmacy in general has been associated with higher caries restoration rates in several studies (Rindal et al. 2005; Maupome et al. 2006; Jurasic et al. 2019). For older adults, polypharmacy should be considered in the assessment of their oral health and risk for oral disease. For more information on multiple medication use and dry mouth, see the section on Salivary Gland Dysfunction and Xerostomia in this chapter.
Ventilator-Associated Pneumonia
Older adults are at increased risk for developing and possibly dying from pneumonia. Ventilator-associated pneumonia (VAP) is an infection occurring in patients receiving mechanical ventilation and is the most common hospital infection associated with intensive care (Hunter 2012). VAP is associated with increased morbidity, mortality, length of stay, antibiotic use, and cost (Rello et al. 2002; Bouadma et al. 2012; Zilberberg et al. 2020), but several preventive approaches exist (Bouadma et al. 2012). Some of these preventive approaches are related to oral hygiene and the reduction of pathogenic oral bacteria. The most recent review on oral hygiene care including the use of prescription antibacterial mouth rinse (chlorhexidine), and the prevention of VAP has indicated some reduction in the development of VAP in critically ill patients (Hua et al. 2016). However, there is no evidence of a difference in the outcomes of duration of mechanical ventilation, length of intensive care, or mortality.
Late-Life Depression
Late-life depression is characterized by feeling sad, an inability to enjoy life, loss of self-esteem, guilt over past minor failings, or thoughts of suicide. This type of depression, reported by 10% of the male and 15% of the female population aged 65 years and older, can easily be masked as a side effect of other health conditions (Federal Interagency Forum on Aging-Related Statistics 2016) and can have a large impact on the oral health of older adults. For example, rampant tooth decay—including decay of the tooth roots—can occur if people lose interest in self-care, increase intake of high-carbohydrate foods, or are treated with medications that cause dry mouth. People with depression report more frequent tooth pain, painful chewing, and bleeding gums—all indicators of poor oral health (Park et al. 2014). They also are prone to periodontitis, which can lead to tooth loss and chewing impairment, affecting a person’s overall quality of life. The number of teeth extracted also is associated with late-life depression. The severity of depression has been associated with the number of missing and decayed teeth, as well as with oral dryness (Skoskiewicz-Malinowska et al. 2018).
Frailty and Morbidity
Frailty is common in older adults and is characterized by an increased risk for poor health outcomes, such as falls, disability, hospitalization, and mortality (Xue 2011). Frail persons require assistance with mobility, suggesting the need for varied assistance with daily activities of life. Of note, frailty is more common among smokers (Kojima et al. 2015).
Global research shows a link between a variety of oral health problems and increased frailty in older age (Ramsay et al. 2018). Specifically, the need for a dental prosthesis was significantly associated with frailty (de Andrade et al. 2013). Tooth loss in healthy seniors has also been associated with mobility, gait instability (Brand et al. 2015), and a future decline in higher-level functional capacity. Treatment for tooth loss has attenuated this functional decline (Sato et al. 2016). A recent systematic review suggests a longitudinal association between oral health and frailty. However, whether oral health is a risk marker or risk factor for frailty remains unclear (Hakeem et al. 2019).
Frail people are at risk for new and recurrent oral diseases, such as root caries, periodontal disease, and fungal infections, stemming from other diseases, medications, and dependency on others for their oral health care. Frail individuals often require assistance with mobility and such activities as personal hygiene and eating. Avlund et al. (2003) reported that, for people 75 to 80 years who have few or no teeth, chewing limitations and mobility problems are interrelated. Thus, mobility problems must be addressed, because fatigued older adults who are dependent on others may not routinely access dental care (Avlund et al. 2003). Furthermore, because they rely on others for help, frail older adults also may have difficulty maintaining good oral hygiene and accessing oral health care, which then increases the risk for declining oral health. The cost of oral health care may be prohibitive in light of their extensive medical needs, and treatment options may be limited for those who are the most frail, especially those with extensive oral disease.
The associations between frailty and oral conditions underscore the importance of the approach developed by the Seattle Care Pathway (Pretty et al. 2014). Specifically, this approach emphasizes intensifying risk-based prevention and improved communication with caregivers to bring older adults to improve and maintain their oral health as frailty develops and dependency increases.
End of Life
Older adults with functional dependence may encounter challenges accessing and receiving appropriate oral health care (van der Putten et al. 2014). The Seattle Care Pathway is an approach that guides practitioners to protect, maintain, and optimize oral health throughout life (Pretty et al. 2014). This clinical pathway requires health professionals to identify a patient’s level of dependency (from no dependency to high dependency) in order to guide assessment, prevention, treatment, and communication protocols (Pretty et al. 2014). This approach is used to develop appropriate treatment plans for independent, healthy older adults, as well as vulnerable adults toward the end of life, with a focus on preparing older adults for increasing dependency and frailty.
At the end of life, terminally ill patients rarely receive oral care because they cannot access dental offices. To address this issue requires an interdisciplinary approach to integrate dentistry into palliative and hospice care. Oral health care providers must use a whole-health approach to understand what type of care is needed and would be the most comfortable for people in their last days. Some have advocated addressing the stages in the death experience—decline, pre-actively dying, actively dying—and the dental care that might be appropriate at each stage, with the goal of promoting comfort, oral function, and quality of life (Chen and Kistler 2015).
Studies identified xerostomia as the most common oral health issue in terminally ill patients; they also face bacterial or fungal infections, oral pain, and prostheses that no longer function (Gordon et al. 1985; Chen et al. 2013a; Chen et al. 2013b; Kvalheim et al. 2016). Many of these issues can and should be treated with comfort-focused bedside care from a dental professional. Although this seems reasonable and empathic, dental students and other oral health professionals need learning opportunities to become comfortable with dying patients and how to manage care in the settings where they reside (Macdonald et al. 2020). This is also discussed in Section 4: Oral Health Workforce, Education, Practice, and Integration.
Mortality
Recent studies suggest an association between the number of missing teeth and mortality—specifically, the higher the number of missing teeth, the greater the risk of mortality (Caplan et al. 2017; Vogtmann et al. 2017; Jansson et al. 2018; Koka and Gupta 2018; Tanaka et al. 2018). A study using U.S. data showed that significant tooth loss (0–15 teeth), root caries, and periodontal disease were associated with higher mortality, and smoking was found to explain the link between mortality and root caries and periodontal disease (Kim et al. 2013). Such relationships are not necessarily causal. Tooth loss and oral disease are more common among those with unhealthy diets and limited access to health care, as well as those who use tobacco products. Those factors, which also place people at higher risk for chronic diseases, are associated with less education and lower incomes (Koka and Gupta, 2018).
Prevention and Management of Oral Diseases and Conditions
Separating the management of oral diseases and conditions in older adults from the management of general health is impossible. Oral and systemic diseases interact in ways that are not always clear. In some cases, systemic diseases influence oral outcomes. In other cases, oral diseases and conditions affect the symptoms and course of other health conditions, such as diabetes, or important daily functions, such as eating. As researchers advance knowledge about these complex relationships, oral health professionals will need to take a more person-centered, holistic approach to providing dental care to people aged 65 years and older.
It has become increasingly clear that general health—especially certain chronic conditions in older adults—influences oral diseases and conditions. Oral manifestations of systemic diseases are common and often are overlooked by medical providers, although there are significant conditions that can have a negative impact on quality of life. Table 2 shows some of these consequences. A medical provider’s inspection of the mouth between the lips and uvula (back of the soft palate) can provide insights into general health. Medications and other treatment of chronic diseases can alter oral health, which may require special interventions to minimize adverse effects. It will be critical for dental and medical providers to work together to identify and minimize the systemic risks to oral health and to appropriately manage oral disease in light of the fact that many older adults develop multiple chronic diseases as they age. The ability of all health care professionals to identify risks for, and signs of, poor oral health is critical for ensuring timely referral for appropriate prevention and management of oral diseases and conditions.
Table 2
Medical conditions with oral health consequences.
Preventive health care typically considers three levels of prevention (primary, secondary, and tertiary). As in the case of working-age adults, the main preventive efforts directed at orofacial diseases in older adults are focused on dental caries, periodontitis, and oral cancer. Primary prevention interventions for dental caries aim to prevent tooth decay from occurring and often include health promotion activities that focus on changing poor dietary habits and encouraging better oral hygiene, including brushing and flossing (National Institute on Aging 2020). The use of fluoride, including varnish or fluoride-containing toothpaste, either purchased over the counter or provided by a dentist as a prescription, also are important primary prevention activities for dental caries. Other important primary prevention efforts include tobacco cessation interventions and substance misuse counseling to prevent periodontitis and other harms to the mouth.
Secondary prevention efforts are intended to detect early signs of disease, generally through receiving regular care, and to reduce the impact of early disease onset. Silver diamine fluoride is an effective chemotherapeutic intervention for managing the impact of dental caries (either coronal or root caries) when the caries process has been limited to a small cavity. A different chemotherapeutic approach to helping to control the progression of gingival inflammation and periodontitis is the use of anti-inflammatory, antibacterial mouth rinses such as chlorhexidine, which is by prescription only. A secondary prevention activity that is generally considered important for oral health is screening for oral and pharyngeal cancers.
The focus of tertiary prevention is controlling the disease after diagnosis to prevent progression to tooth loss or to provide rehabilitation to restore some function that facilitates quality of life. For controlling caries progression in adults, a variety of restorative options are available. In controlling periodontitis, the objective is to prevent bone loss by using a variety of nonsurgical therapies and periodontal surgery, if necessary. For oral and pharyngeal cancer, the objective is to intervene early with surgery, radiation, and/or chemotherapy to reduce mortality and impact on quality of life.
Prevention and Management of Dental Caries
Management of caries in healthy older adults follows the same principles of risk assessment, prevention, and minimally invasive care for working-age adults, as noted in Section 3A (Hayes et al. 2020). However, for older dependent adults, management of caries may be affected by physical and cognitive impairments, as well as intraoral and extraoral risk factors that are unique to older adults (Boehm and Scannapieco 2007). One important aspect of caries prevention for older adults with comorbidities lies in making them aware of the particular risk factors that result from their diseases and the medications used to manage them. A wide range of medications cause dry mouth, increasing the risk for caries, but individuals may be unaware of the risk. They may even be unaware that there has been a change in their salivary flow, and consequently unaware that their preventive routine may need to change.
Root exposure as an age-prevalent condition in older adults leaves them vulnerable to root caries in particular, although caries commonly occurs on other surfaces as well. Root caries also is distinct from coronal caries, with several important differences from the caries process to appropriate therapies (Damé-Teixeira et al. 2017). Because root caries is more prevalent in older adults, early detection is important to long-term control and management of the disease. However, the use of diagnostic tests, beyond the standard use of a dental explorer to detect caries, is unable to provide any additional benefit for the detection and diagnosis of root caries (Fee et al. 2020). Topical fluoride applications can be effective in preventing root caries (Zhang et al. 2020b).
A caries risk assessment is a helpful precursor in determining risk-based treatment options, which may include such products as prescription-strength fluoride rinses and gels, salivary substitutes, and stimulants for home use. These may be combined with oral hygiene aids, such as electric toothbrushes and floss holders for the individual or a caregiver. For older adults with dental caries, the use of conventional restorative treatments (fillings, etc.) versus strategies that may include incomplete caries removal and atraumatic restorative techniques (ARTs), such as silver diamine fluoride (SDF) and conventional glass ionomer cement, is dependent on the extent of tooth decay and a person’s ability to tolerate traditional restorative techniques.
For adults with a medical condition that impacts their ability to receive or access care, caries management may include glass ionomer restorations, interim therapeutic restorations, or ARTs. However, while the evidence to support the use of these minimally invasive treatment procedures for children is substantial, evidence for use in adults is limited (Dorri et al. 2017). Another minimally invasive procedure that has recently emerged to arrest or slow the advance of caries until the patient is able to receive definitive treatment is the application of SDF (Hendre et al. 2017; Oliveira et al. 2018). For some people at the end of life, any of these measures can also be provided as an element of palliative care to prevent the need for more extensive restorations or reduce the risk of an acute event that could result from untreated and advancing caries, such as tooth pain, infection, or tooth fracture (Boehm and Scannapieco 2007; Hayes et al. 2020).
Prevention and Management of Periodontal Disease
Periodontal disease often is associated with other comorbidities in older adults. For those who are healthy or for those with well-controlled systemic disease(s), treatment options and outcomes of treatment could be anticipated to be the same as for younger adults (Boehm and Scannapieco 2007; Renvert and Persson 2016). For those with multiple or poorly controlled systemic disease, treatment options may be limited, and outcomes of treatment may be compromised. People with a variety of medical conditions also use multiple medications, many of which can impact periodontal health, from diminished salivary flow (Wolff et al. 2017) to gingival hyperplasia (Aral et al. 2015). Further, the risk factors for many noncommunicable diseases and poor oral health, including periodontal disease, often are shared, such as poor nutrition, smoking, substance abuse, and limited health literacy or access to care. Such risks may be compounded by physical or cognitive impairments, resulting in refractory or advancing disease (van der Putten et al. 2013; Renvert and Persson 2016).
These risks must be identified and discussed with the patient or caregiver in order to develop a treatment plan and achieve the best outcomes in care. In some cases where a patient cannot or will not comply with recommendations to address modifiable risk factors, options for management may be limited to nonsurgical approaches, and success of treatment may be limited (Boehm and Scannapieco 2007).
For persons who are moderately to highly dependent on others for the tasks of daily living, a palliative approach focused on preventing progression of disease and maintaining dentition may be indicated (Boehm and Scannapieco 2007). Maintaining periodontally involved dentition may be of particular importance if this dependency also limits options for tooth replacement. Further, because periodontitis has been identified as a risk factor for many noncommunicable diseases, maintenance of the periodontium is critical. Periodontal treatment that reduces bacterial load is of particular importance for frail older adults. Because poor oral hygiene has been shown to be associated with aspiration pneumonia in this population (Loeb et al. 1999), addressing this is important. Establishing an individualized plan for daily oral hygiene, prevention, and maintenance to mitigate risks from systemic diseases and medications that can directly or indirectly affect oral health is critical for older adults with systemic disease and some level of dependency, and especially for persons who are most vulnerable because of frailty and high dependence (Boehm and Scannapieco 2007).
Management of Tooth Loss
Healthy older adults who have lost teeth can benefit from the full array of replacement options as described in Section 3A. Options will vary with changes in health status or level of dependency. For persons with no or low dependency issues, a full range of options is viable, with appropriate risk/benefit awareness from the patient, based on their specific conditions. For example, a patient with diabetes should be informed of the potential for oral infections if their diabetes is not well controlled. Once a disease and disability has begun to impact access to care and even the oral cavity directly—from dry mouth to diminished oral hygiene—options for replacement may become more limited. As dependency increases, maintaining function is critical, but less invasive procedures and easily cleansable fixed or removable prostheses or a shortened dental arch may need to be considered (McKenna et al. 2020). For individuals at the highest levels of dependency, tooth replacement may no longer be an option, and the primary goal will shift to general comfort of the oral cavity and maintenance of any existing dentition with adequate daily oral hygiene measures and regular preventive care (Boehm and Scannapieco 2007).
Oral Health Literacy
Health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (Ratzan and Parker 2000). Adults with higher health literacy make better choices about their care, disease-prevention activities, health behaviors, and interactions with the health care system.
Health literacy is a resource. Like other resources, health literacy skills are not evenly distributed across the population. The National Assessment of Adult Literacy estimates that only 12% of the population is “proficient” in prose, document, and quantitative abilities (Kutner et al. 2006), meaning that the vast majority of Americans do not have the skills necessary to effectively respond to the complex requirements needed to understand the U.S. health care system. Older adults typically have lower average health literacy compared to younger adult age groups, and only 1 in 20 older adults had the skills to fully understand and communicate health-related information (Kutner et al. 2006). Oral health literacy among older adults was a concern communicated by the Surgeon General during a 2004 Senate Committee hearing on Aging and Health Care (2003). One study using community-based geriatric rotations involving dental students and community-dwelling older adults observed some improvements in oral health literacy as a result of the interactions between older adults and dental students (Hjertstedt et al. 2014). It is clear, however, that more work is needed to improve the oral health care system and oral health literacy to better meet the needs of older adults. More information on oral health literacy is presented in Sections 1 and 3A.
Special-Needs Populations
Older Adults with Disabilities and Special Health Care Needs
The majority of older adults in the United States use traditional settings for oral health care, such as private practices, community health clinics, and government-funded health centers. For adults of all ages, financial barriers such as low income, lack of insurance, and lack of transportation can limit access to oral health care. However, as medical, cognitive, functional, and behavioral challenges arise and dependence increases, additional constraints develop. In addition, individuals with developmental disabilities are aging at unprecedented rates and have unique health and service needs (Factor et al. 2012). Of the 49.2 million U.S. adults aged 65 years and older in 2016, 8.3 million (16.9%) required long-term care, including adult day care (0.6%), residential care (1.6%), hospice care (2.9%), nursing home residence (2.7%), and home health care (9.1%) (Harris-Kojetin et al. 2016). These individuals require some assistance with the activities of daily living, including daily oral care and accessing regular dental care. Chronic medical conditions, along with a reduced capacity for self-care, increases their risk for caries, periodontal disease, and oral pathology.
Often people with special needs, the medically compromised, and those who are older are considered “extreme caries risk,” which by definition is a high-risk person who also has diminished salivary flow. This is an age-prevalent condition for older adults who may take several medications that result in diminished salivary flow, leading to multiple advanced caries lesions (rampant decay)—especially on root surfaces in older adults with recession—or to periodontal attachment loss.
Additional specific risk factors exist for this population. Some people may have poor oral hygiene as a result of some physical (e.g., severe arthritis, cerebral palsy, or Parkinson’s disease) or cognitive impairment (e.g., Alzheimer’s disease or vascular dementia). Some individuals may require special diets—such as soft, pureed, or thickened liquids—because of a gastrointestinal or swallowing disorder, or even due to poor oral health. These situations, in turn, place them at risk for caries because of the difficulty of removing such foods from the tooth surfaces and, for some, a reliance on others to perform oral hygiene (Chavez et al. 2018).
For people with a limited ability to cooperate for care, it also is important to note that behavioral techniques can be used to provide preventive and restorative care. A wide array of sedation options also are available, from oral to intravenous sedation and general anesthesia for persons with advanced dental needs and limited to no ability to cooperate because of physical or cognitive limitations. An interdisciplinary approach to treatment planning in these complex cases is critical to determine the patient’s ability to tolerate and benefit from the proposed treatment and method of delivery (Chavez et al. 2018). Due to the many coexisting risk factors within vulnerable populations, some may be at risk for rapid deterioration of their oral health because of a combinations of factors related to their general health. These factors can include sensory loss or change, polypharmacy, the presence of disease (e.g., Parkinson’s disease or diabetes), or physical or cognitive impairment following a stroke. Other factors can include social support needs (reliance on caregivers, living situation, palliative care status, or finances) as well as their oral condition (past dental history, current oral hygiene status, and oral mucosal conditions). A Rapid Oral Health Deterioration Assessment of these three domains has been developed by Marchini and colleagues (2019b) to aid in appropriate treatment planning and intervention for these at-risk individuals. Four risk categories are defined in this assessment, and it is important to note that caries prevention is included in all four levels because caries is a leading cause of such rapid deterioration.
Issues of Abuse and Neglect
Ten percent of vulnerable older and disabled adults are estimated to be at risk for abuse and neglect, although this number is believed to be underreported. Abuse and neglect can be intentional (active) or nonintentional (passive) and can include neglect of oral health and trauma to the head and neck (Petti 2018). Individuals dealing with depression or dementia also can be at high risk for self-neglect. There may be a reluctance to report suspected abuse. Evidence may be attributed to, or confused by, findings that might otherwise be associated with aging or disability, such as bruising related to medication use or trauma; or from falls or other accidents as a result of vision, gait, or balance impairments. Identification of abuse and neglect also may be a challenge for persons with cognitive impairments who cannot clearly relay information or for persons who may be dependent on the abuser and fearful of making a complaint (Evans et al. 2017; Chavez et al. 2018; Centers for Disease Control and Prevention 2020b).
Homebound and Frail Older Adults
Homebound adults face high risks to their oral health (Crete et al. 2018), as well as greater rates of disease, frailty, and physical limitations that lead to dependence (Ornstein et al. 2015; Norman et al. 2018). In 2011, about 2 million community-dwelling older adults were homebound and in need of home-based care because of declines in physical and/or cognitive health (Ornstein et al. 2015). These adults live in the community with varying degrees of dependence, based on their physical, psychiatric, and/or social ability to leave home (Crete et al. 2018). In dentistry, the functional ability of an older adult is based on his or her ability to travel to a dental office, seek services independently, and perform oral health care (Table 3).
Table 3
Functional ability for aging older adults applied to oral health care.
High-dependency individuals—people who cannot be transported or moved—must receive dental services in their home or a long-term care facility (Pretty et al. 2014). Recent studies categorize homebound adults using three main measures: homebound (in the last month, never left home or went out once a week or less); mostly homebound (went out once a week or less); semi-homebound (could leave home, but with the risk of becoming homebound due to a disease, symptom burden, or impairment creating a challenge; or if they need personal aid to leave home); and non-homebound (Cohen-Mansfield et al. 2012; Ornstein et al. 2015) (Figure 10). Although a great number of homebound individuals are older, some younger individuals are homebound as a result of developmental and other disabilities (Special Care Dentistry 2002).
Figure 10
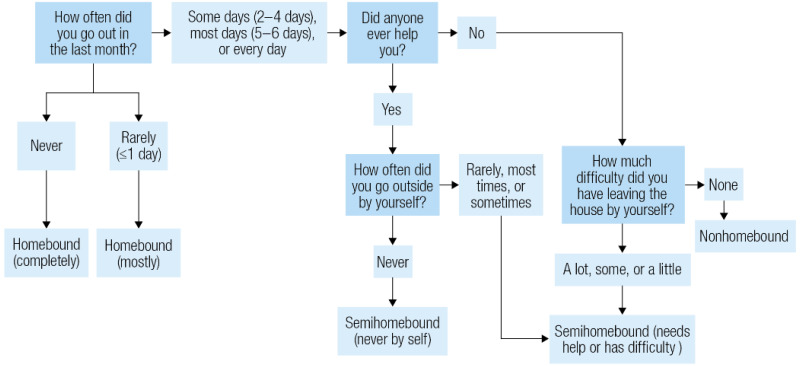
Determining homebound status using the National Health and Aging Trends Study. Note: Respondents were asked a series of questions as part of a Mobility Questionnaire found in the National Health and Aging Trends Study.
Compliance with regular dental visits is more difficult for homebound adults because of their social and physical challenges. A large proportion of homebound and semi-homebound adults have not seen a dentist in two or more years (Crete et al. 2018). Deterioration of oral health can be rapid and severe in the absence of routine care (Gluzman et al. 2013; Norman et al. 2018). Dental caries, periodontal disease, tooth loss, and the use of prostheses are basic indicators of poor oral health among older adults (Dye et al. 2015; Muller et al. 2017). The presence of untreated oral diseases can have a negative impact on quality of life, general health, well-being, and nutritional status.
For these reasons, routine dental visits for homebound adults are required to maintain good oral health and detect oral and systemic conditions and diseases early (Chamut et al. 2021).
A 2011 Institute of Medicine report recommended that general health care professionals take a more active role in the dental care of adults living in long-term care facilities (Institute of Medicine and National Research Council 2011). The report suggested that such professionals assess risk and screen for common oral conditions, educate patients about how to prevent oral diseases (e.g., daily brushing with fluoride toothpaste), and deliver preventive services (e.g., fluoride varnish, silver diamine fluoride).
Oral Health and Quality of Life
Good oral health is an important aspect of quality of life (Jones et al. 2006). Van de Rijt and coworkers (2020) conducted a systematic review to identify oral health factors associated with oral health–related quality of life (OHQoL) in people 65 years and older.
They found that a functional dentition, oral pain, and functional complaints are all positively associated with OHQoL. Jones et al. (2002) showed that the single-item self-report of oral health (How would you rate the health of your teeth and gums?) using a Likert scale 5-item response (excellent, very good, good, fair, or poor) could accurately identify persons in need of dental care.
Dental Service Utilization
Older adults living in poverty are less likely to utilize the oral health care system, which contributes to the persistent oral health disparities observed in the United States. In 2017, 2 in 3 older adults had a dental visit in the past 12 months. Older adults who were either poor or close to poverty (43%) were less likely to have had a dental visit, compared with nonpoor (74%) older adults (Kramarow 2019). Non-Hispanic White older adults were more likely to have had a dental visit in the past year (69.1%), compared with Hispanic (54.7%), non-Hispanic Black (52.6%), and non-Hispanic Asian (52.8%) older adults. A recent survey of American Indian/Alaska Native/Native Hawaiian elders representing all regions of the United States and 262 tribes reported that nearly 57% of the older adult population had a dental visit in the past year (Schroeder et al. 2019).
Older adults with some natural teeth are more than twice as likely to have had a dental visit in the past 12 months (73.6%), compared to those with complete tooth loss (30.3%). About 8% of adults 65 years and older needed dental care in the past 12 months but did not get it because of cost. Older adults (65 years and older) who were poor or close to poverty were more likely to have an unmet need for dental care because of cost (14%), compared with nonpoor older adults (5%) (Kramarow 2019).
Among the elderly, dental utilization strongly correlates with dental insurance coverage. Two-thirds of older adults with private dental insurance have had a dental visit in the past 12 months, whereas only one-third who are uninsured had a dental visit. For those older adults with some public insurance, fewer than 15% had a dental visit in the past 12 months (Nasseh and Vujicic 2016). Among the four major age groups representing the lifespan, older adults are most likely not to have dental insurance (57%); they also spent the most out-of-pocket for dental care (see Section 1 Figures 13–14 in this monograph for more information).
Provision of Older Adult Oral Health Care in Alternative Settings
Alternative Models
Alternative models of care are required for older adults with severe impairments who are no longer able to come to a dental clinic. Examples include mobile practices and virtual dental homes using teledentistry. The latter allows care to reach people in long-term care facilities, senior centers, and other places where seniors normally congregate, as well as at home. A mobile practice can range from a mobile van equipped as a dental clinic to portable equipment brought to the patient’s bedside (Langelier et al. 2017). Given the costs of transporting staff and equipment, the mobile model is a more costly alternative to an office visit. Virtual dental examinations have been shown to be an acceptable alternative to in-person examinations (Namakian et al. 2012). The virtual dental home is “based on the principles of bringing care to places where underserved populations live, work, or receive social, educational, or general health services, integrating oral health with general health, social and educational delivery systems, and using telehealth technologies to connect a geographically distributed, collaborative dental team, with the dentist at the head of team making decisions about treatment and location of services” (Glassman 2012a). See Section 4 for a discussion of telehealth technologies in dentistry.
Chapter 2. Advances and Challenges
The oral health of Americans 65 or older has improved significantly during the past 2 decades. Older Americans now have fewer teeth extracted, and the proportion with complete tooth loss (edentulism) is at an all-time low. Much of this improvement in tooth retention can be attributed to a greater focus on prevention and advances in treating and preserving teeth affected by dental caries and periodontal disease. Changes in attitudes, such as decreased social acceptance of tooth loss and decreased smoking rates, as well as improved awareness of the benefits of oral health, also have contributed to more older adults keeping more teeth than in any previous generation. Challenges to improve oral health in older adults remain, and barriers to achieving oral health care continue. The single most important barrier is the affordability of dental insurance and dental care, as many U.S. adults lose their employee benefits when they retire. Increases in tooth retention and the acquisition of dental implants by more older adults make ongoing preventive care very important for this age group.
Etiology and Prevalence of Oral Diseases and Conditions
Dental Caries
Overall, the prevalence of untreated decay in adults aged 65 and older has declined 6 percentage points since 2000, from approximately 28% to 22% (Figure 11). Men have experienced a significant decrease in untreated dental caries (32% to 25%), but prevalence still remains higher for men than for women (25% vs. 20%). There have been decreases in the prevalence of untreated caries for non-Hispanic Blacks and Mexican Americans aged 65 and older, but the decrease among older non-Hispanic Black adults has been the highest, especially for those 75 and older. Nevertheless, disparities remain (Figure 12). Unfortunately, untreated caries did not significantly decrease for older adults age 65 and older living in poverty (48% to 43%) or for more affluent older adults (21% to 14%), with the disparity being greatest among those 75 and older (Figure 13).
Figure 11
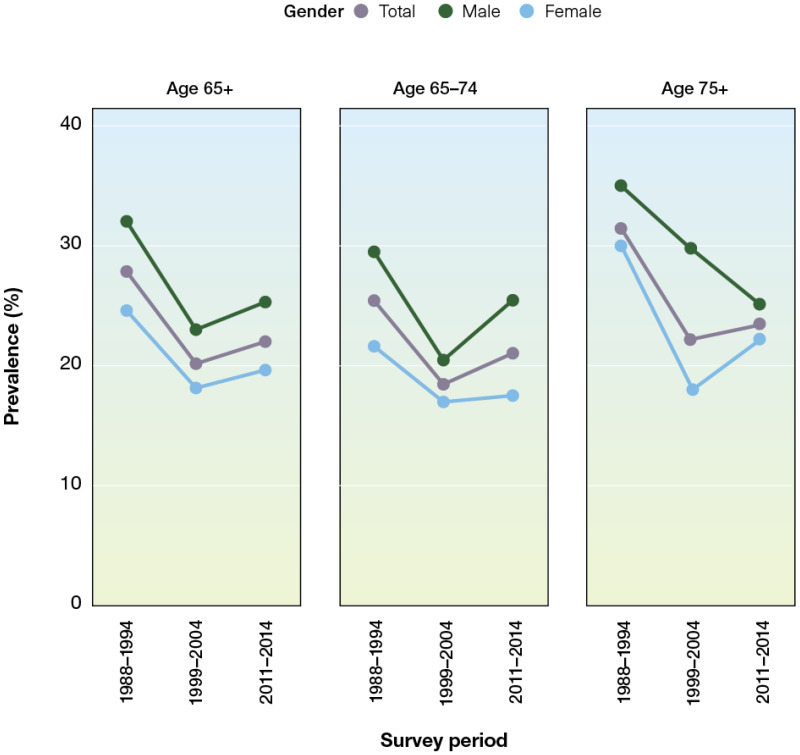
Percentage of adults ages 65 and older with untreated dental caries in permanent teeth by age group and gender: United States, 1988–1994, 1999–2004, 2011–2014. Note: Prevalence of untreated dental caries in permanent teeth (DT (more…)
Figure 12
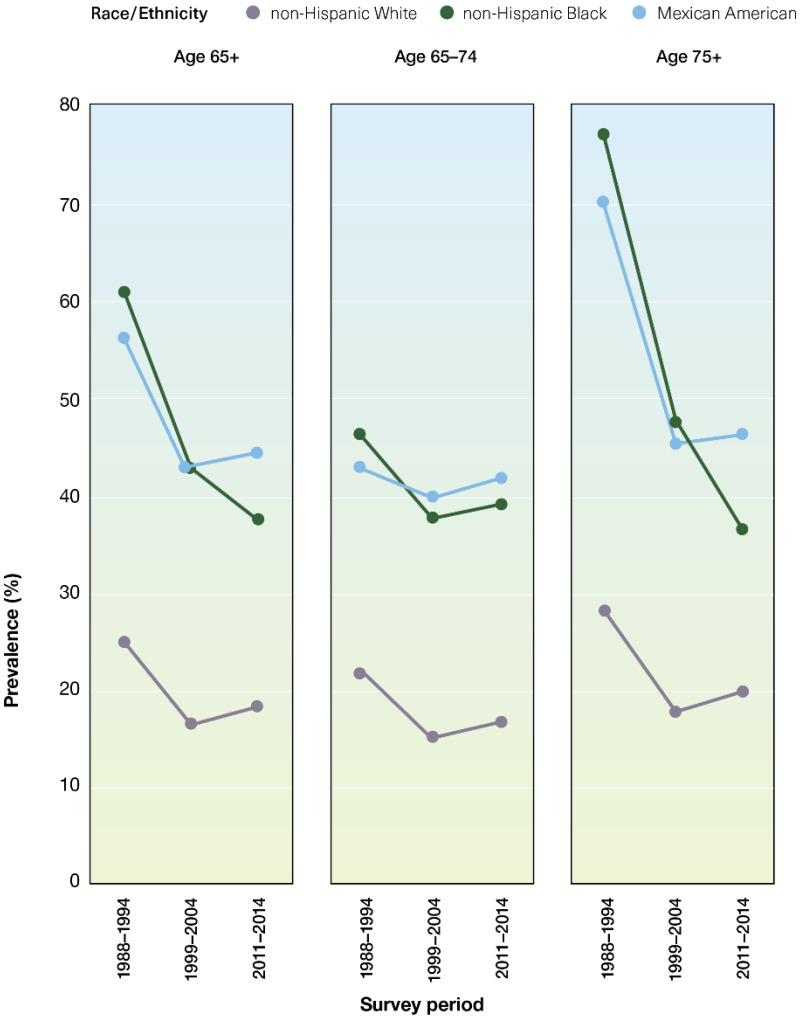
Percentage of adults ages 65 and older with untreated dental caries in permanent teeth by age group and race/ethnicity: United States, 1988–1994, 1999–2004, 2011–2014. Note: Prevalence of untreated dental caries in permanent teeth (more…)
Figure 13
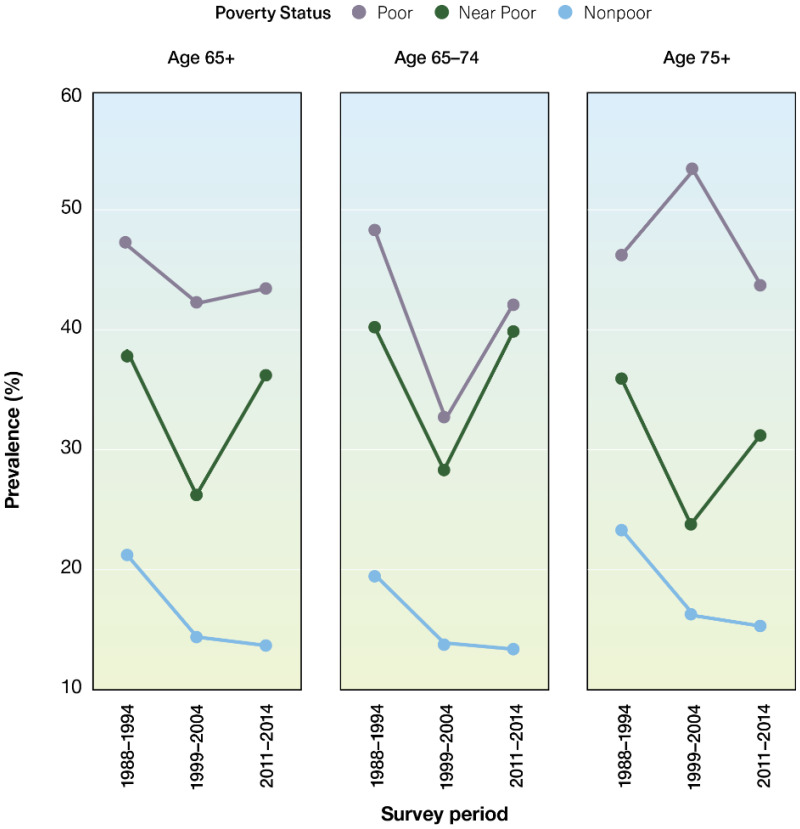
Percentage of adults ages 65 and older with untreated dental caries in permanent teeth by age group and poverty status: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Prevalence of untreated dental caries in permanent teeth (more…)
Although the prevalence of dental caries has changed little among older adults since the 2000 report (96% to 97%), another measure of dental caries experience has significantly changed. During the last 2 decades, the mean number of decayed, missing, and filled teeth (DMFT) has decreased from about 19 teeth affected by dental caries to 17 teeth affected by dental caries (Figure 14). This decrease has been driven by a substantial reduction in the mean number of missing teeth, declining from about 10 missing teeth to fewer than 7 missing teeth. Interestingly, this substantial increase in the mean number of teeth not extracted also parallels a significant increase in the mean number of teeth restored. Since the turn of the century, the mean number of teeth with dental fillings and crowns increased for older adults from about 9 to 10 teeth. Paradoxically, the mean DMFT for older adults living at 200% of the federal poverty guideline or higher has declined from 19 to 17 teeth affected by dental caries; but for those older adults living in poverty, the mean number of teeth affected has remained unchanged (about 18).
Figure 14
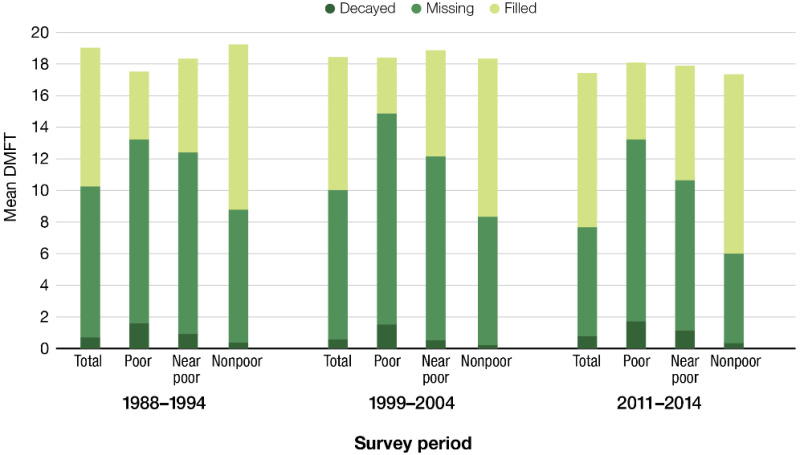
Mean DMFT for adults ages 65 and older by poverty status: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Mean DMFT = Sum of the means of decayed (DT), missing (MT), and filled (FT) permanent teeth, FPG = Federal Poverty (more…)
For older adults living in poverty, the mean number of teeth lost due to dental caries decreased from about 12 to 11 teeth during the past 2 decades, and the mean number of teeth with dental fillings and crowns increased from nearly 4 to 5. However, for those living at 200% of the federal poverty guideline or higher, the mean number of missing teeth decreased from about 8 to 6 teeth, with the mean number of teeth restored increasing from about 10 to 11 teeth.
Changes in DMFT by race/ethnicity indicate that disparities remain, although some indicators show improvement. For example, among non-Hispanic Blacks, the mean number of missing teeth decreased from about 14 to nearly 11 on average, whereas for non-Hispanic Whites, the decrease was from about 9 to 6 missing teeth (Figure 15). For Mexican Americans, the decrease was from about 10 to 9 mean missing teeth. Although non-Hispanic Black and White older adults have seen a reduction in the number of teeth affected by dental caries over the past 2 decades, Mexican American older adults have not.
Figure 15
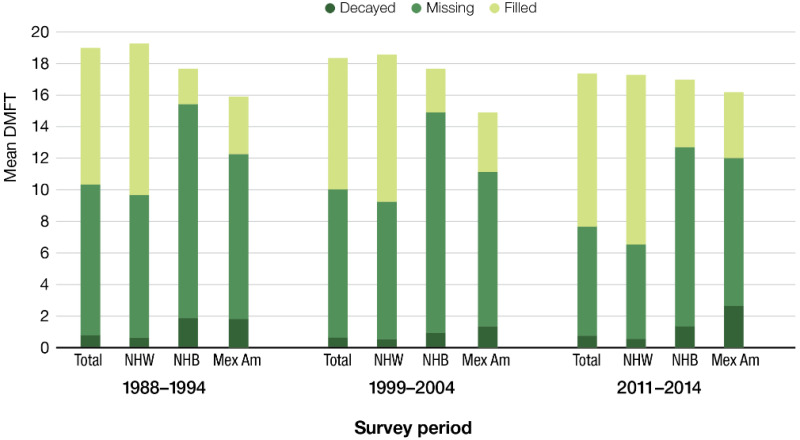
Mean DMFT for adults ages 65 and older by race/ethnicity: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Mean DMFT = Sum of the means of decayed (DT), missing (MT), and filled (FT) permanent teeth. NHW = non-Hispanic White, (more…)
Overall, these changes show that there has been some improvement in dental caries experience (DMFT) for some older adult groups, but substantial disparities remain. Clearly, older Americans living in poverty have not experienced the same kind of reduction in the prevalence of dental caries compared to more affluent older Americans.
Periodontal Disease
With nearly 1 in 10 Americans aged 65 years and older experiencing severe periodontitis (Eke et al. 2018), periodontal disease in this age group is an important public health problem that needs to be addressed. People who are poor, with fewer years of education, and who are Hispanic or African American, are at increased risk for severe periodontitis (Borrell and Crawford 2008; Eke et al. 2016b). These individuals have reduced access to oral health care services, and approaches to close this gap must be developed (Seo et al. 2019). Moreover, measures that are used to assess the prevalence and severity of periodontitis, such as clinical loss of attachment or gingival recession, increase with age, which clearly demonstrates that older age is an important risk indicator for periodontitis (Billings et al. 2018). As gingival recession increases, dental roots become noticeable, and exposure to dental caries on tooth roots becomes greater.
As the U.S. population ages and more older adults retain more teeth, they become more susceptible to periodontitis and its complications. In addition to the local effects of severe periodontitis, including discomfort, abscess formation, masticatory inefficiency, reduced quality of life, and tooth loss, the potential impact on general health is another important consideration. As a result, the dental profession will be required to provide dental care to people with more complex health histories who may have a reduced capacity to tolerate dental care and who take a range of medications that have direct and indirect effects on the oral cavity, including xerostomia (Barbe 2018).
Salivary Gland Dysfunction and Xerostomia
Over the past 20 years, progress has been made in better understanding salivary gland dysfunction and xerostomia (dry mouth). These conditions now can be described and measured more specifically than before, resulting in more valid and reliable estimates of their occurrence. There also is considerable evidence confirming the major impact of dry mouth on day-to-day lives, with this condition being one of the most common reported factors in oral health–related quality of life (OHRQoL). The role of various drugs and associated polypharmacy in causing dry mouth also is better understood and is the most common cause of xerostomia in older adults.
Whenever possible, reducing or modifying medication routines can help to lower the prevalence of xerostomia. Raising awareness among health professionals, including physicians, nurses, and pharmacists, about the negative oral health effects of dry mouth due to polypharmacy remains a challenge (Marcott et al. 2020). Older adults admitted to the hospital should be asked about dry mouth as part of the standard medical history obtained at hospital admission.
Current challenges for conducting research on and treating dry mouth include obtaining valid, reliable, and representative data on salivary flow rates; understanding the natural history of dry mouth; and managing polypharmacy at the population level. Measuring salivary flow rates in epidemiological studies is difficult and time consuming. Researchers would benefit from a standardized saliva collection technique for population studies because there is no current guidance in the most widely used oral epidemiology manual (World Health Organization 2013). Understanding the natural history of dry mouth requires data from prospective cohort studies, particularly studies that measure both xerostomia and salivary flow. Little is known about how the condition manifests throughout the life course. Data from some cohort studies of older adults have shown variable degrees of incidence and resolution over time (Locker 1995; Thomson et al. 2006c; Johansson et al. 2009; Enoki et al. 2014), but the knowledge base for younger or middle-aged adults is limited.
Loss of Teeth
Edentulism, the loss of all natural teeth, decreased from about 32% to 17% among adults aged 65 and older over the past 20 years (Figure 16). Among those 75 and older, substantial declines in edentulism also were observed, with a decline from about 38% to 22% overall.
Figure 16
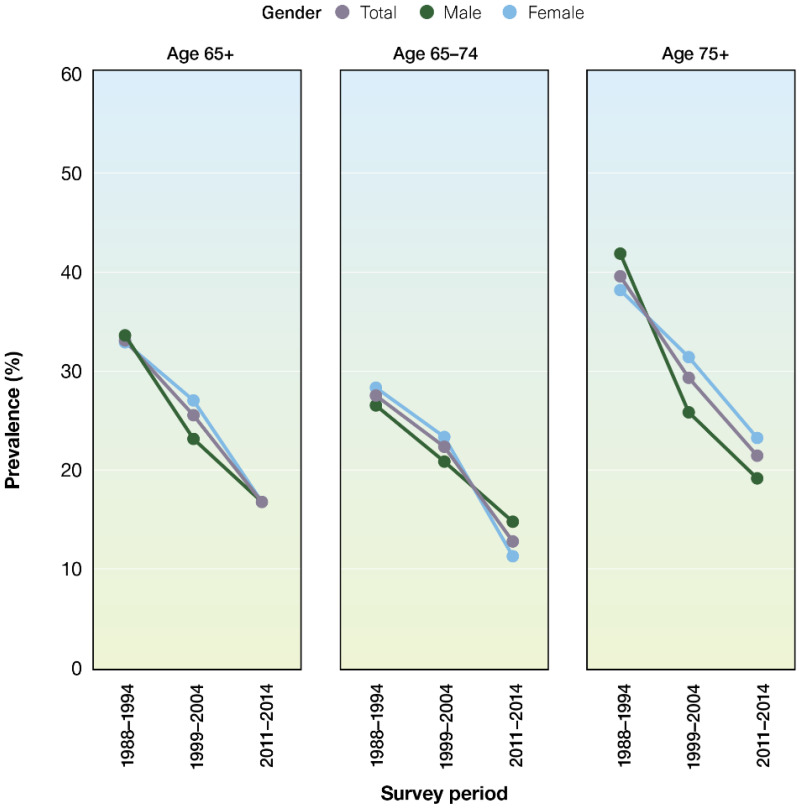
Prevalence of edentulism among adults age 65 years and older by age group and gender: United States, 1988–1994, 1999–2004, 2011–2014. Note: Edentulism is complete loss of all natural permanent teeth.
Edentulism has declined substantially for all older Americans, regardless of sex, race/ethnicity, and poverty. For example, among older non-Hispanic Black adults, edentulism decreased from 37% to 26% and from 51% to 33% for those age 75 and older (Figure 17). Significant improvements were observed for older adults living in poverty (45% to 30%) and for adults age 75 and older living in poverty (51% to 36%) (Figure 18).
Figure 17
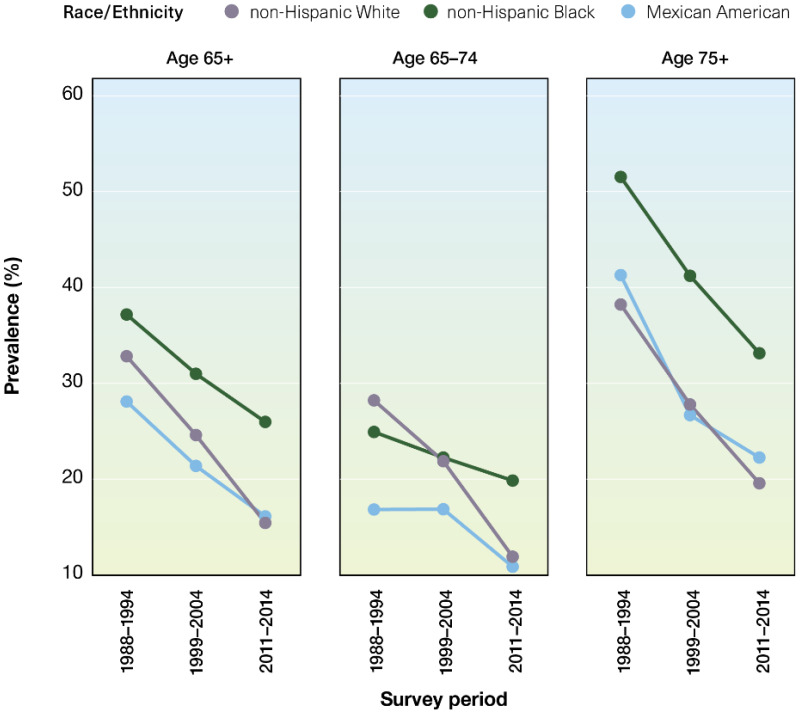
Prevalence of edentulism among adults age 65 years and older by age group and race/ethnicity: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Edentulism is complete loss of all natural permanent teeth.
Figure 18
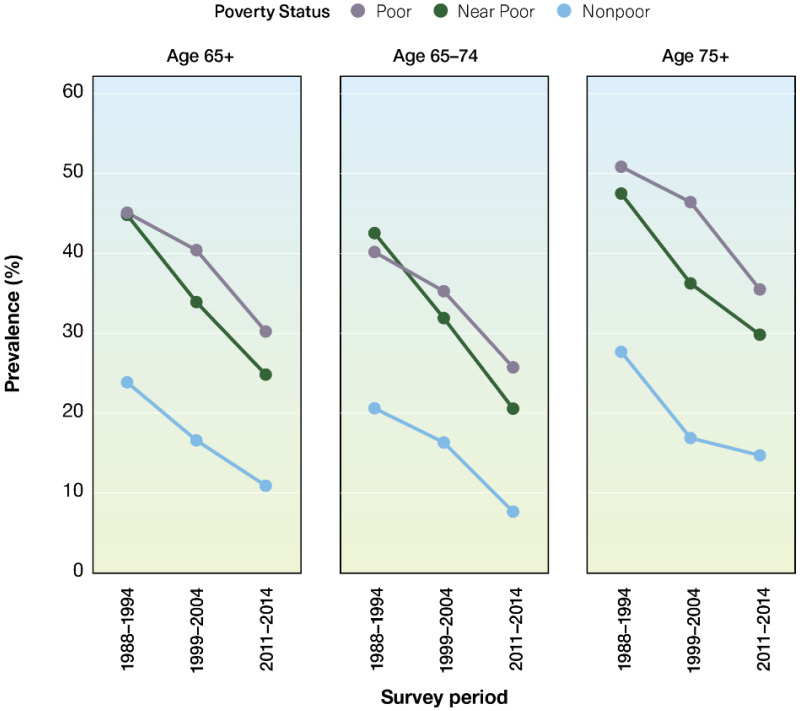
Prevalence of edentulism among adults age 65 years and older by age group and poverty status: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Edentulism is complete loss of all natural permanent teeth; FPG = Federal Poverty (more…)
The prevalence of older adults aged 65 to 74 years with a complete dentition has improved over time, doubling since the year 2000, from about 8% to 17% (Figure 19). However, this good news is tempered by the significant increase in disparities based on race/ethnicity and poverty status. Substantial increases have occurred for non-Hispanic Whites (improving from 8% to 20%), but the increase observed for non-Hispanic Blacks was not significant (3% to 5%), and there was no change for Mexican Americans in this age group. Although increases observed across poverty strata were significant for all groups since 2000, disparities between the poor and the more affluent older adults aged 65 to 74 years have increased.
Figure 19
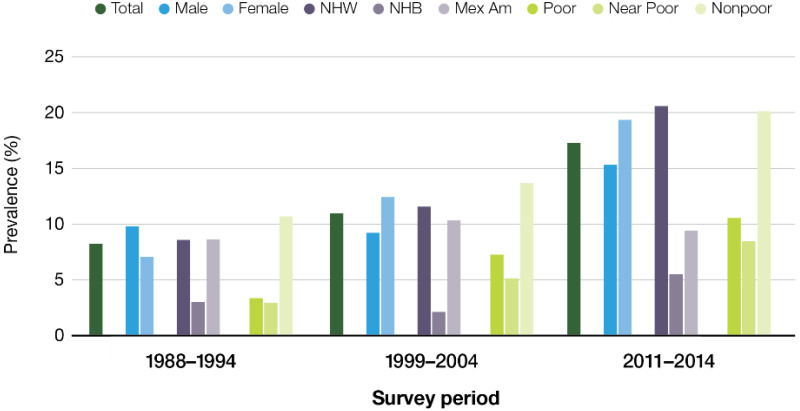
Percentage of adults ages 65–74 with a complete permanent dentition by gender, race/ethnicity, and poverty status: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Complete dentition is having all natural teeth remaining (more…)
Having a functional dentition (more than 20 teeth) also has improved markedly among older adults since the publication of the 2000 report on oral health, increasing from 46% to 65% (Figures 20–22). Improvement was observed across sex, racial/ethnic, and income groups. Although key subgroups of older Americans experienced significant increases, substantial disparities observed at the time of the last Surgeon General’s Report on oral health in 2000 did not improve during the last 2 decades. For example, although non-Hispanic Blacks and Mexican Americans improved from 24% to 33% and from 38% to 49% respectively, because, non-Hispanic Whites improved from 48% to 72%, the observed disparity for this important oral health metric worsened during the last 2 decades.
Figure 20
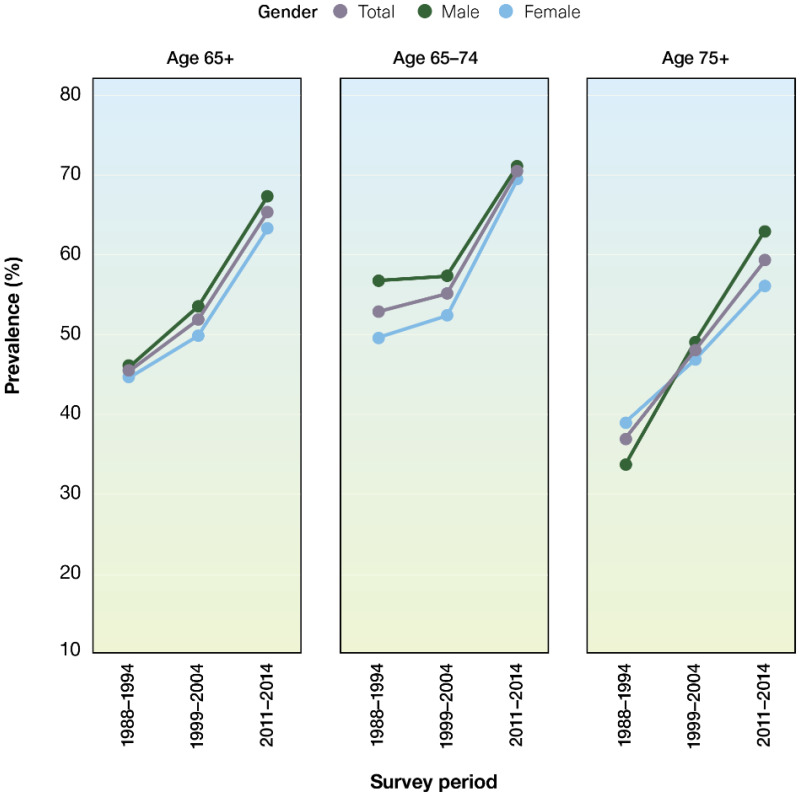
Percentage of adults age 65 years and older with a functional dentition by age group and gender: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Functional dentition is having 21 or more permanent teeth remaining, excluding (more…)
Figure 22
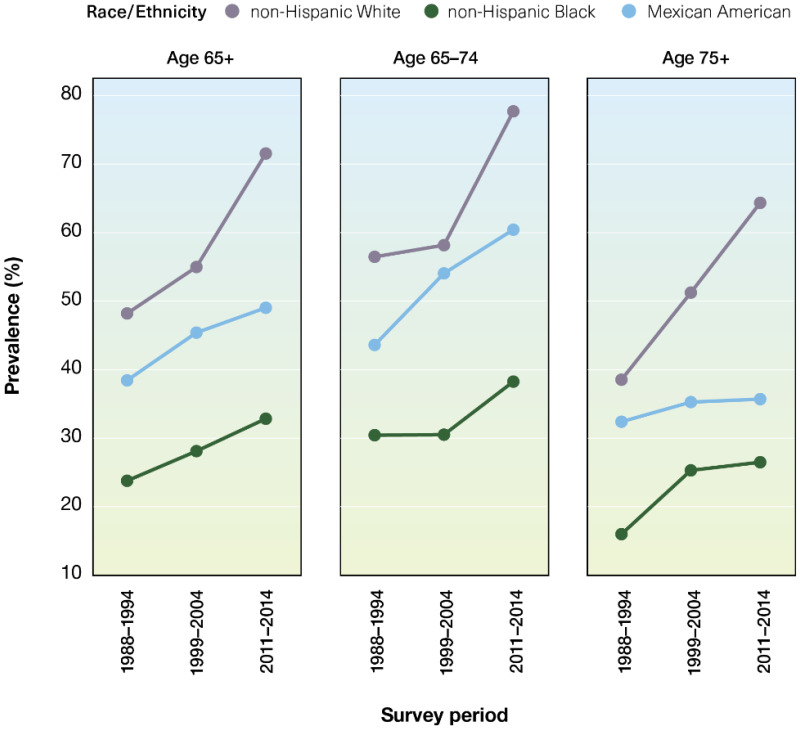
Percentage of adults age 65 years and older with a functional dentition by age group and race/ethnicity: United States, 1988–1994, 1999–2004, 2011–2014. Note: Functional dentition is having 21 or more permanent teeth remaining, (more…)
Differences by income were even more pronounced. For all older Americans living in poverty, the prevalence of having a functional dentition increased from 32% to 41%. However, prevalence increased from 52% to 74% for older, nonpoor Americans. Among older adults age 75 and older, there was no significant improvement for those living in poverty (29% vs 35%), whereas there was substantial improvement for nonpoor adults age 75 and older (44% vs 69%) (Figure 21).
Figure 21
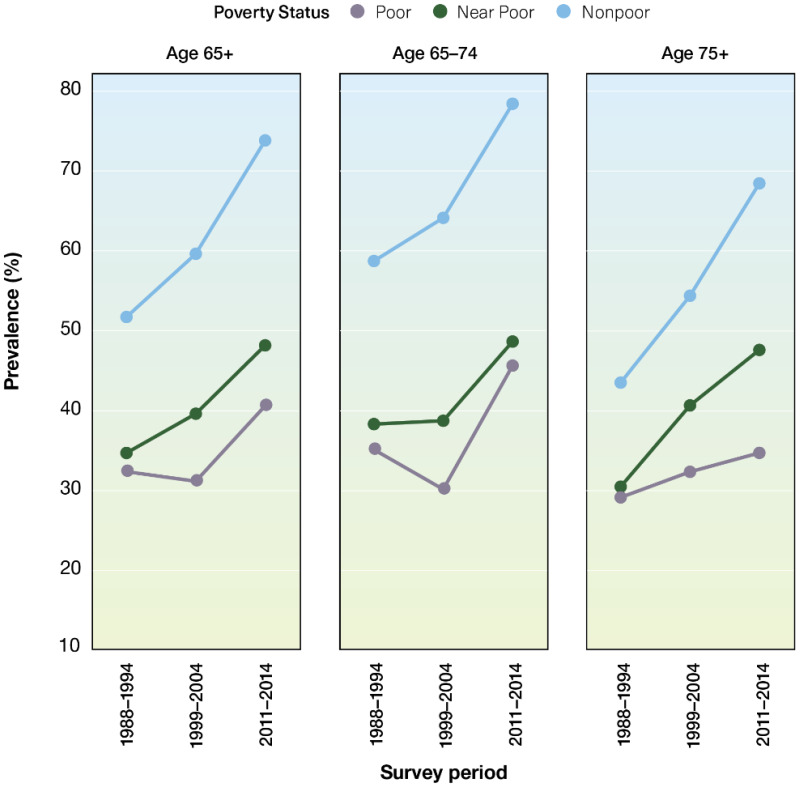
Percentage of age 65 years and older with a functional dentition by age group and poverty status: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Functional dentition is having 21 or more permanent teeth remaining, excluding (more…)
High-Risk Behaviors Affecting Oral Health in Older Adults
Dietary Behaviors, Nutrition, and Food Insecurity
Oral health and nutrition are interrelated challenges for older adults (Gerontological Society of America 2020). The associations between tooth loss (with or without dentures), cognition, diet, nutrient intake, and nutrition status are multidirectional and become even more complex for older adults who are managing multiple comorbidities. As oral health declines, individuals might not even realize they are making changes to their diet by choosing softer, less varied, and less nutritional foods that can present a risk to their dentition and health.
Both oral and systemic conditions can impact dietary choices and dictate food texture (Chavez et al. 2018). People who have had a stroke or have Alzheimer’s disease, for example, may have chewing and swallowing problems that restrict their diet to soft textures or thickened liquids. These types of diets, combined with increased frequency of intake over the day, can present a challenge to oral hygiene and the prevention of caries and periodontal disease progression. When the diet is altered specifically because of dental pain or missing teeth, then restoration of the dentition could resolve the issues, and diet could be improved. Older adults can experience changes in smell or taste that are associated with normal aging; or they may result from dental disease, oral pathology, or the use of multiple medications. Such chemosensory changes can affect enjoyment of food and, subsequently, nutritional status (Chavez et al. 2018).
Social and economic issues may be at the center of nutritional deficiencies in older adults (Gerontological Society of America 2020). For those who rely on social opportunities to access a nutritious meal, social isolation can affect their nutritional status. Identifying and making an appropriate referral for assistance can be an important element of care for those who lack access to nutritious meals as a result of eating alone, have a limited ability to shop, or experience difficulty preparing meals for themselves. This can be as important as restoring a dentition that may be a source of embarrassment for an older individual who might be isolating as a result. Many older adults with limited incomes who suffer disproportionately from oral and systemic diseases also may experience food insecurity (Gerontological Society of America 2020). Referral to appropriate social services or enlisting the help of family or friends—with the individual’s permission, or even through Adult Protective Services in cases of abuse or neglect—are important opportunities for intervention that can occur when oral health providers are an integral part of a larger interdisciplinary team (Chavez et al. 2018). Effective approaches are needed to manage the impact of medications or of nutritional deficits on oral health, as well as tooth loss and/or tooth replacement on diet, nutrition status, and the eating experience.
Social Determinants of Health
Older adults who are disadvantaged or marginalized face additional challenges. For example, among hundreds of factors considered, emotional and systemic factors—such as chronic stress and limited health literacy—were the strongest predictors of self-reported poor dental health among urban Hispanics (Yoon et al. 2018). Older American Indian/Alaska Native adults, many of whom live in rural communities with limited transportation, also face emotional and systemic factors that contribute to persistent poorer oral health compared to the general U.S. population.
The lack of research on social inequities among older adults has been recognized in regard to overall health. The National Institute on Aging, for example, published a report in 2015 detailing a framework for health disparities research, particularly on older adults (Hill et al. 2015; National Institute on Aging 2018). In 2017, to address this lack of focus, the National Institute of Dental and Craniofacial Research encouraged partnerships among researchers in aging and oral health disparities and interdisciplinary research collaborations to address disparities among older adults (Fischer et al. 2017).
Interrelated Effects of Oral Health with General Health
The scientific literature exploring the relationships between oral health and general health has grown substantially during the past 20 years. Overall, the literature suggests an important relationship between chronic oral infection/oral inflammation as a result of periodontal disease and the risk for some noncommunicable diseases, primarily cardiovascular disease, diabetes, respiratory disease, and cognitive impairment. A growing body of evidence implicates inflammation as playing an important role in this relationship, particularly with the association between cardiovascular disease and periodontitis (Carrizales-Sepúlveda et al. 2018). Emerging research is now pointing to the possibility of a hyperactive immune response occurring after an overabundant production of a particular type of white blood cell, or neutrophils, in response to bacterial infections responsible for periodontitis (Fine et al. 2021). There continues to be a need to define the relationship between periodontal disease and systemic health.
Furthermore, the knowledge gathered over the past 2 decades indicating an association between various dental conditions and diabetes, cardiovascular disease, and cancer also have underlying effects related to poor nutrition. An almost century-old hypothesis on nutrition is gathering support: nutritional interventions associated with improved oral health may reduce the risk for some non-oral chronic diseases. A review by Moore and colleagues (2018) of nutrition and cognitive decline and late-life depression concluded that B vitamins, n-3 polyunsaturated fatty acids, and polyphenols may exert strong protective effects in preserving cognition and preventing depression. Conducting clinical research to identify effective dietary interventions is an ongoing challenge, but it is essential for discovering new and promising preventive interventions directed toward reducing the U.S. burden of chronic noncommunicable and dental diseases.
Prevention and Management of Oral Diseases and Conditions
Since the publication of the 2000 Surgeon General’s Report on oral health, evidence-based approaches to treatment planning and management of oral diseases and conditions in older adults have emerged. The Seattle Care Pathway is designed as a pragmatic approach to care for older adults based on a variety of factors, starting with assessing patients’ functional status and then considering the potential risks to their oral health (Pretty et al. 2014). There are essentially five functional categories, with each having a set of prevention and treatment recommendations that is appropriate for each category (Table 4).
Table 4
Seattle Care Pathway (SCP) overview.
Many older adults experience difficulties in self-care and access to care, placing them at higher risk for oral diseases. Even something as basic as brushing one’s own teeth and flossing may not be possible because of arthritis or the tremors of Parkinson’s disease, for example. The use of electronic brushes and prethreaded floss, over-the-counter fluoride rinses, and prescription gels (1.1% NaF) are helpful. Yet, as people become more frail and dependent, they may require the assistance of a home health aide or family caregiver. Regular, more frequent professional care also may be needed, especially in persons who regularly experience dental decay or have periodontal disease, dental prostheses, or dental implants. Addressing many of these needs requires facing persistent and complex challenges that can be compounded when retired adults lack the financial resources to receive regular oral health care.
Management of Tooth Loss and Replacement with Dental Implants
Dental implant technology has markedly improved in the past 2 decades. Improved materials, procedures, and provider experience have made it possible for adults to replace missing teeth with implants faster and with higher success rates than ever before. Contemporary dental implants that are finished with a crown (Figure 27 in Section 3A) or a denture are very durable and aesthetically realistic. Their success rates are typically among the highest of any type of surgical implants. The survival rate of implant-supported dentures after 25 years is greater than 80% (Frisch et al. 2020). In addition, it was reported that most implants did not develop signs of periodontal inflammation around the implant (peri-implantitis) over the same time period. More information on dental implants is presented in Sections 3A and 6 of this monograph.
Because of improved durability, aesthetics, and support, dental implants are becoming the preferred treatment for many older adults who can afford them. During the last 2 decades, the prevalence of dental implants has increased from about 1% to more than 7%. (Figure 23). In addition, older adults are three times more likely to have a dental implant, compared to working-age adults. Older adults have an average number of 2.4 dental implants. This number has remained consistent as the percentage of older adults with a dental implant has increased.
Figure 23
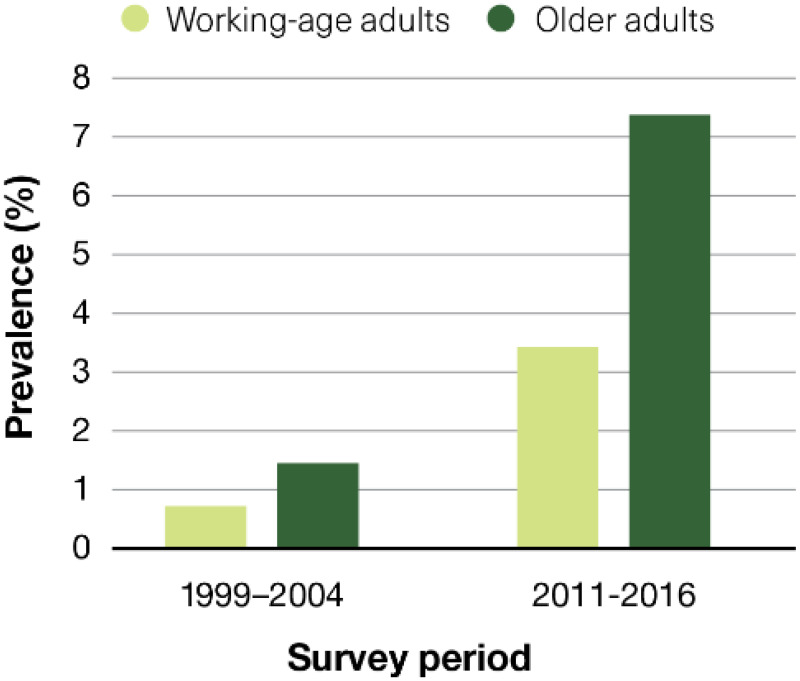
Percentage of adults age 20 and older with at least one dental implant: United States, 1999–2004 and 2011–2016. Note: Working-age adults are ages 20–64 years; older adults are age 65 and older.
Managing Salivary Gland Dysfunction and Xerostomia
Dry mouth is difficult to treat. The available therapies aim for palliation (symptom relief), stimulation (of salivary flow), and regeneration (of secretory tissue). The approach taken depends on whether dry mouth is due to medications, radiotherapy, or Sjögren’s syndrome (Table 5). The past 20 years have seen more randomized, controlled clinical trials of interventions for the relief of dry mouth, enabling systematic reviews to determine their efficacy. To date, four Cochrane reviews involving 87 studies (Furness et al. 2011; Furness et al. 2013) have been undertaken. Slightly more than one-third of these studies were assessed as being at high risk of bias, indicating a need for better quality studies and more careful reporting. Even so, those reviews have been useful in assessing the likely efficacy of the various therapeutic and preventive approaches.
Table 5
Overview of evidence for the various therapies for dry mouth.
While there is no sound evidence yet for the efficacy of medication review in treating medication-induced dry mouth, consistent evidence about the role of polypharmacy in causing dry mouth suggests a logical starting point. Oral health professionals, medical providers, and community pharmacists working together could raise awareness of dry mouth and ensure that affected individuals are managed and advised in a timely and appropriate manner. The evidence for palliation using water sprays, chewing gum, and sucking lemon drops remains relatively weak, although these options may be useful for some individuals.
Topical lemon and citric acid can stimulate salivary flow, but excess use can result in the erosion of dental enamel. Systemic pilocarpine or cevimeline has been effective (Brimhall et al. 2013).
Patients who have undergone radiotherapy to the head or neck are at particular risk of dry mouth. While this is far less common than the medication-induced condition, it presents a clinical problem that severely compromises quality of life. Accordingly, therapeutic approaches have received greater research attention. Investigations of palliative approaches have used a range of methods—saliva substitutes, chewing gum, and water—but the evidence for their effectiveness remains weak. Stimulation using systemic pilocarpine has been effective, but not without side effects. The evidence for effectiveness is weaker for electrical stimulation and the medication bethanechol. Artificial saliva products face challenges in matching the consistency and properties of human saliva.
Gene therapy and stem cell therapy interventions have been investigated using animal models, but there is little progress to date. For Sjögren’s syndrome, the evidence is weak for palliation using saliva substitutes. Gene therapy and stem cell therapy interventions have been investigated using animal models. Saliva-restoring gene therapy clinical trials currently are being conducted. However, the evidence is relatively strong for stimulation using systemic sialogogue, pilocarpine, and cevimeline (National Institute of Dental and Craniofacial Research 2018; Chiorini 2020).
Finally, managing dry mouth requires attention to the dentition and its supporting structures, including the oral mucosa. Preventing dental caries is an important part of such management and involves twice daily use of fluoride toothpaste and the avoidance of nonmilk extrinsic sugars (such as sugary beverages or sugar added to coffee), along with more intensive preventive measures, such as prescribed fluoride (1.1% NaF, 5500 ppm F) or mouth rinses, where appropriate. In older adults, dry mouth also can affect denture retention, and patients may need to use denture adhesives (Ship and Hu 2004). Not only can there be problems in retaining and using partial dentures, but the remaining natural teeth—especially abutment teeth—may be at increased risk of dental caries. Although the long-held assumption that older people taking xerogenic medications are at higher risk for caries has not thus far been supported by epidemiologic evidence (Thomson et al. 2002), prudence dictates the assumption that people who take many medications are at increased risk for dry mouth.
Managing Effects of Oropharyngeal
Cancer Treatments
Efforts to Reduce Illness from Radiation Therapy
Radiation therapy affects normal tissue in the field of radiation by causing rapid cellular turnover in bone or soft tissue. The long-term side effects from radiotherapy include salivary gland hypofunction and dry mouth, resulting in extreme risk for dental caries. There also is the potential for osteonecrosis of the jaw related to radiation therapy and high-dose bisphosphonate/antiresorptive therapy, which may be administered intravenously to prevent or manage bony metastasis, as well as trismus (lockjaw) that severely limits oral range of motion, severe mucositis (ulceration and irritation of the oral mucosa), and significant tissue defects resulting in functional changes (Vissink et al. 2018). Trismus affects 23–45% of individuals who undergo radiation therapy and can significantly impact the muscles involved in chewing (Brennan et al. 2008). Development depends on such factors as age, dentition, primary cancer site, free-tissue transfer, re-irradiation, and chemotherapy (Rapidis et al. 2015). These conditions can result in significant short- and long-term or even permanent pain and discomfort, and have adverse impacts on nutritional intake, speech, and swallowing, as well as oral hygiene practices and OHRQoL. Aggressive preventive measures and frequent dental visits are required to prevent deterioration of the oral cavity, which can occur rapidly.
A major shift over the past 20 years has been how radiation therapy is delivered. Intensity-modulated radiation therapy (IMRT) was invented in 1996 to treat prostate cancer, with the goal of minimizing radiation to healthy tissue. IMRT was modified for the treatment of oropharyngeal cancer (OPC) using a parotid-sparing protocol (Murdoch-Kinch et al. 2008; Duarte et al. 2014). The goal was to save at least one of the parotid glands to decrease the degree of salivary gland hypofunction, minimize risk for osteoradionecrosis (ORN), or destruction of bone due to radiation, and reduce other tissue involvement that could increase discomfort and risk discontinuing radiation. Future goals are to increase radiation distribution precision and to more clearly identify the amount of radiation received in dental areas (Tsai et al. 2019).
Reducing Extractions and Osteoradionecrosis
The traditional standard of care has been to act aggressively in removing diseased teeth prior to radiation therapy to minimize the risk for ORN, should extractions be needed at a later date. Before the turn of the century, it was highly likely that multiple extractions would occur due to the poor condition of the dentition and the high risks of decay and potential ORN. Poor condition of the dentition often was associated with the risk factors of the cancer—smoking and alcohol use—and patients typically reported minimal use of routine dental preventive services. Now that OPC is increasingly related to human papillomavirus (HPV), more individuals who receive radiation treatment have fewer dental problems and a history of regular dental care. Knowing that teeth can be maintained because of a reduced risk of ORN and the availability of preventive measures, such as silver diamine fluoride (Strohl et al. 2019), medical indication to remove teeth prior to radiation therapy has decreased.
The timing of extractions also has been studied, with the goal of maximizing the time between extractions and the start of radiation to allow for maximum wound healing (Strohl et al. 2019). This typically requires advanced communication and a team approach between the oncology and dental teams, which is a best practice. Ineffective or no collaboration may result in the need for multiple sessions requiring general anesthesia, resulting in additional costs and risks. The currently established interprofessional head and neck cancer team (dental, oncology, ENT, radiation) approach should be implemented nationwide to maximize individualized patient care. Implementing patient-specific plans would avoid aggressive extraction approaches and serve to better maintain the patient’s quality of life. Strategies for team approaches should be investigated to improve long-term outcomes.
Oral Rehabilitation
Significant developments in both microsurgical techniques and osseointegration have generated new strategies for managing surgical defects after cancer surgery. Prior to 2000, mandibular surgery resulted in a continuity defect, in which the remaining mandible was unsupported and provided little potential for function. Today, mandibular defects are routinely reconstructed with soft or hard tissue, resulting in significant potential for function (Likhterov et al. 2019; Patel et al. 2019).
Survivors of Other Cancers
Over the past 20 years, oncologists and oral surgeons have identified the potential for osteonecrosis of maxillofacial bone in patients who have received intravenous bisphosphonate therapy for metastatic cancer, as well as in those who received radiation therapy. In addition, the potential impact on mucosa and salivary glands from graft versus host disease after a bone marrow transplant has been recognized.
Special Needs Populations
Older adults with disabilities and special health care needs continue to face challenges in obtaining oral health care, including physical disabilities, transportation challenges, and financial limitations. The development of a sustainable, interdisciplinary system of medical and dental care for older adults continues to be a priority. Progress in integrating oral hygiene care with home health care and mobile care provided collaboratively by dental team members is beginning to show promise (Langelier et al. 2017).
Homebound Older Adults
Advances in medicine and dentistry and better disease management have improved older adults’ tooth retention and OHRQoL. Nevertheless, certain problems—namely, dental caries, periodontal disease, and tooth loss—are presumed to persist, especially among vulnerable and homebound older adults (Muller et al. 2017). In general, there is limited information about rates of tooth decay and edentulism among homebound people because of their living arrangements, the absence of a consistent definition of “homebound,” and this population’s reluctance to participate in household studies (Holm-Pedersen et al. 2015). Homebound and disabled individuals are perceived to have a high need for dental care but face multiple barriers in accessing care. Improving access to care requires an array of trained, community-based health providers and advocates who understand the importance of oral health, make appropriate referrals, and provide appropriate care for this population (Special Care Dentistry 2002; Ghezzi et al. 2017).
Unless dental care is delivered in their homes, access may be a problem for homebound elders living in urban areas. The issue becomes even more complex for people who live in rural or isolated areas, where distances are longer and health networks and support services are scarce (Holm-Pedersen et al. 2015). Gluzman and colleagues (2013) found that 92% of 125 homebound individuals in their study needed dental treatments beyond oral hygiene, and that 96% indicated that they had not seen a dentist since they became homebound.
Chamut and colleagues (2021) assessed dental visits in the past 12 months among community-dwelling adults who received home- and community-based services (HCBS), administered under the Older Americans Act. Among the five HCBS programs studied—case management, homemaker services, congregate meals, home-delivered meals, and transportation—the groups receiving case management and home-delivered meals, on average, had fewer annual dental visits. Low educational attainment (less than high school diploma) was the strongest indicator for not having had a dental visit (Chamut et al. 2021). Researchers also found that the oldest participants (aged 85 or older) who received home-delivered meals and transportation were more likely to have had a dental visit (Chamut et al. 2021). As an increasing number of older adults retain more of their teeth, meeting the needs and demands for oral care of this population will require additional resources and a skilled dental workforce that is an integral part of the health care system (Thomson and Ma 2014).
The failure to provide regular and preventive oral health care for this population underscores a major gap in the interprofessional model of health care, which does not routinely include oral health care providers (Holm-Pedersen et al. 2015; Critchlow 2017). A transformation of the oral health care system will be required to deliver dental care and prevent oral disease in this difficult-to-reach group, which also receives little attention from policymakers in regard to oral health (Thomson and Ma 2014).
Nursing homes and other long-term care facilities have a limited capacity to deliver needed oral health services to their residents, most of whom are at high risk for oral diseases (Dye et al. 2007). Although nationally accepted guidelines for anticipatory guidance and risk assessment and management—including oral health guidelines—are the standard of care in pediatrics, the adoption of similar standards for oral health in elders is lacking.
Figure 25
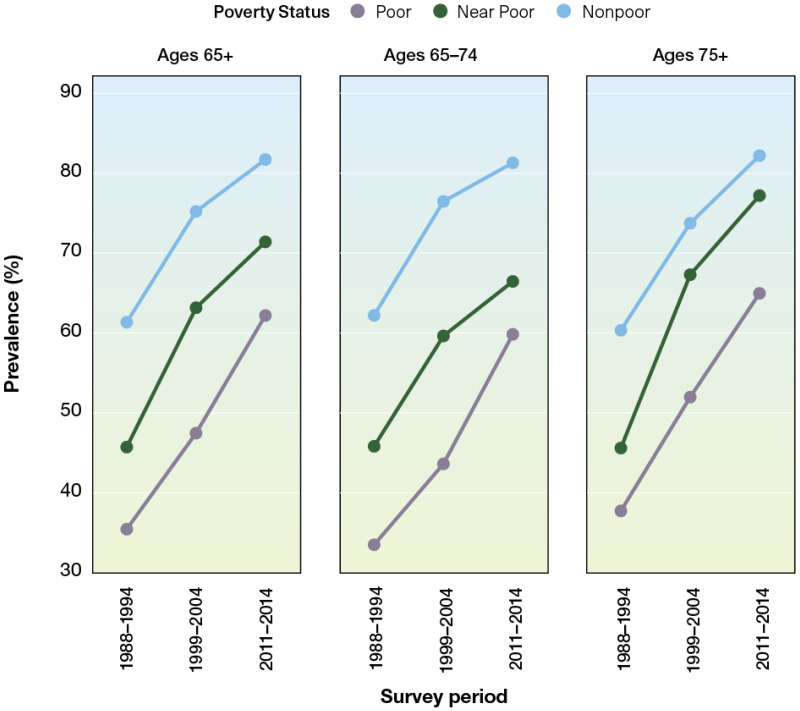
Percentage of adults age 65 years and older reporting overall satisfaction with their teeth and mouth by age group and poverty status: United States, 1988–1994, 1999–2004, 2011–2014. Notes: FPG = Federal Poverty Guideline; < (more…)
Having guidelines for this population would facilitate an enhanced focus on older adult oral health and ensure that persons who cannot access oral care receive annual dental and oral cancer screenings, referrals, and prevention services, such as dental cleanings (teeth and dentures) and fluoride applications.
Systems of Care for the Frail Elderly
Studies indicate that current models are not meeting the need for oral care for older, frail adults. Analyses of insurance claims have shown that preventive dental care in older adults with chronic disease is cost-effective (Pourat et al. 2018). However, prospective studies (Sloane et al. 2013) to validate such programs do not exist at a scientific level comparable to geriatric medicine. As a result, the field lacks essential data and evidence-based programs. Critical evaluations are needed for existing models (e.g., inadequate and untrained workforce, limited reimbursement, lack of prevention), promising models (e.g., Program of All-Inclusive Care for the Elderly), and potential workforce models (e.g., role of dental therapists, expanded role for dental hygienists, inclusion of an oral health benefit in Medicare) (Haber et al. 2015).
Because the removal of cost and insurance barriers promotes the use of dental services by older adults (Lee et al. 2015; Slavkin 2017), the addition of an oral health benefit in Medicare would improve access to care nationwide, especially for low-income older adults and those of some racial/ethnic groups. A Medicare dental benefit also might facilitate evidence-based models of comprehensive care, similar to those in geriatric medicine. In 2020, a national coalition of more than 132 stakeholders from dentistry, aging, health care, and industry announced their support of Medicare coverage for medically necessary oral and dental health therapies. Federal legislation will ultimately be required to remove language that excludes the provision of most dental services from Medicare (Chavez et al. 2017).
Another challenge is the insufficiency of the dental workforce to fully address oral health care for older adults. A committee sponsored by the Institute of Medicine (2008) envisioned a future health care system for older adults in which health needs are addressed comprehensively, services are provided efficiently, and patients are encouraged to be active partners in their care. In addition, professional education needs to address the changing environment in which oral health professionals will be needed to provide services. For example, delivering dental care to older, frail adults will increasingly need to occur outside of the traditional dental setting. Moreover, oral health professionals will be called upon to have a greater role in collaborative, palliative, end-of-life care, and current limited training opportunities for the oral health workforce require expansion (Macdonald et al. 2020). This vision of comprehensive medical and dental care remains a viable goal that can be achieved with the right policies and training.
To improve the dental care workforce, the Institute of Medicine committee proposed enhancing geriatric competence, increasing recruitment and retention, and redesigning models of care (Institute of Medicine and National Research Council 2011). The traditional dental workforce—including dentists, dental hygienists, and dental assistants—is not currently able to manage the care of all U.S. older adults. New models are needed to expand the workforce, both within and outside the dental profession. In many states, new and expanded roles are being defined for dental hygienists and dental therapists; their training, licensure, and scope of practice vary by state. In addition, community liaisons and community health coordinators are being trained to address oral health issues as part of their whole-person assessments. Other medical professionals—such as physicians, nurses, occupational therapists, physical therapists, long-term care staff, and social workers—are also targeted for additional training.
Interprofessional education and collaborative clinical practice are needed to create a competent clinical workforce to provide oral health care to older adults. The Geriatric Research Education and Clinical Centers (GRECC) have a long-standing model of interprofessional care in the Veterans Health Administration system (U.S. Department of Veterans Affairs 2021). Development of guidelines and toolkits for education, as well as implementation of care using the GRECC model at a national level, are needed but will require the necessary funding. See Section 4 for more information on issues of integration affecting special adult populations.
Oral Health and Quality of Life
As noted throughout this monograph, oral health problems can significantly affect quality of life. For example, tooth loss and other oral conditions in older adults can affect eating and, by extension, nutritional status. Progress in understanding and treating specific conditions can alleviate problems with oral function and maximize OHRQoL. During the past 20 years, older adults have been feeling more satisfied with the overall condition of their teeth and mouth, with 77% reporting satisfaction, compared to 54% 2 decades ago (Figures 24–26). Non-Hispanic Black and White older adults reported substantially improved satisfaction (33% to 65% and 57% to 81%, respectively), whereas Mexican Americans reported the smallest improvement in satisfaction (32% to 45%), with the majority remaining unsatisfied with the condition of their teeth and mouth. Among those 75 years and older, satisfaction has improved during the last 20 years, but significant differences in oral health satisfaction exist by race/ethnicity and income. Although satisfaction improved for Mexican American adults aged 75 and older, the majority remain unsatisfied with the condition of their teeth and mouth (55%). Among those aged 75 and older living in poverty, satisfaction improved substantially, rising from 38% to 65%.
Figure 24
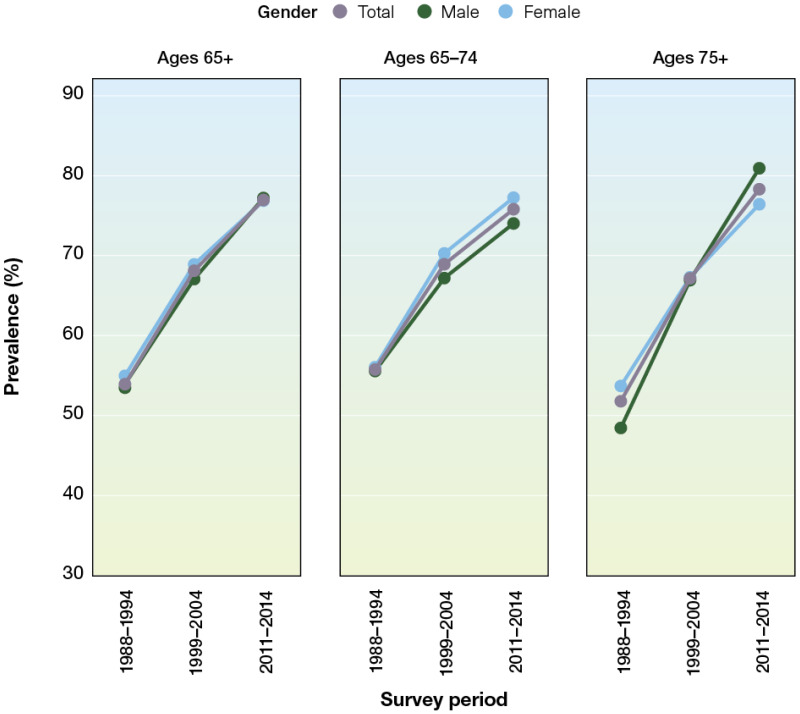
Percentage of adults age 65 years and older reporting overall satisfaction with their teeth and mouth by age group and gender: United States, 1988–1994, 1999–2004, 2011–2014. Note: Overall satisfaction is a self-report of excellent, (more…)
Figure 26
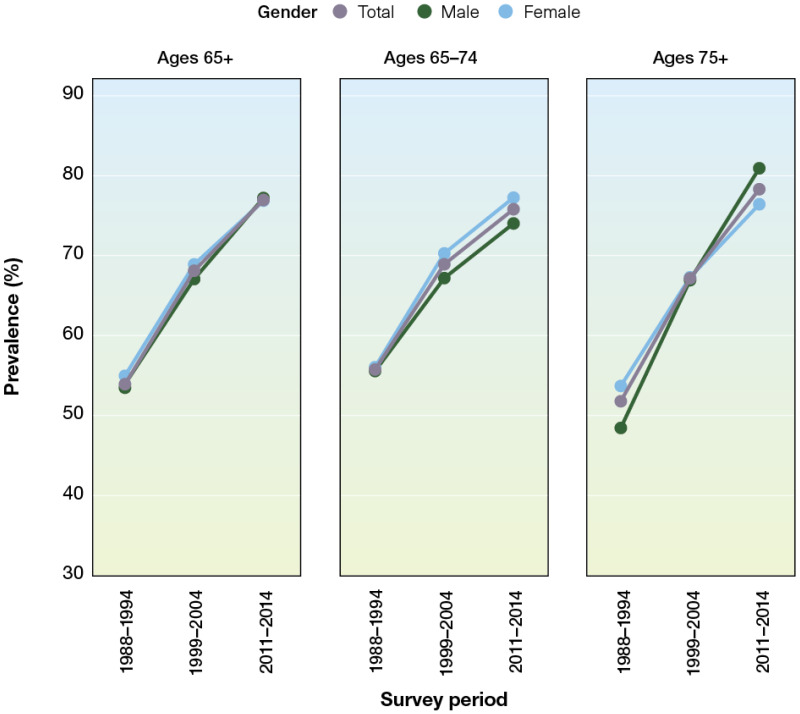
Percentage of adults age 65 years and older reporting overall satisfaction with their teeth and mouth by age group and race/ethnicity: United States, 1988–1994, 1999–2004, 2011–2014. Notes: Overall satisfaction is a self-report (more…)
Cognitive decline affects daily function and is a common cause of social challenges and poor quality of life in older adults. Prevention and treatment of cognitive impairment are becoming increasingly important, given the aging population. Over the past 2 decades, considerable advances have been made in understanding the relationship between tooth loss and impaired cognitive functioning (Onozuka et al. 2002a; Gatz et al. 2006; Hirano et al. 2008; Ono et al. 2010), as well as the more general impact of oral health on cognitive function (Onozuka et al. 2002a; Gatz et al. 2006; Hirano et al. 2008; Ono et al. 2010). Several factors are associated with oral health status, including tooth loss, decreased mastication (chewing) and the resulting impact on sensory stimulation of the brain, poor nutritional pathways, and the role of periodontal disease (Cerutti-Kopplin et al. 2016).
In terms of tooth loss, human neuroimaging studies demonstrate that chewing is associated with activation of brain areas associated with memory and learning, increased cerebral blood flow, and better cognitive performance (Onozuka et al. 2002b; Miyamoto et al. 2005; Lin et al. 2017). These findings suggest a link between mastication and cognition. Prosthetic rehabilitation of toothless persons improved cerebral blood flow, indicating a possible protective influence of masticatory activities on cognitive functioning (Miyamoto et al. 2005). Recent work by Thomson and Barak (2021) suggests using a life-course approach to examine the apparent association between tooth loss and cognition.
Dental Services Utilization
During the past 20 years, the percentage of adults 65 or older who had a dental visit in the past 12 months has increased from 38% in 2000 to more than 44% in 2016 (Nasseh and Vujicic 2016; Yarbrough and Vujicic 2019). During this period, only about 1 in 4 poor older adults had a dental visit. Interestingly, the percentage of older adults with private dental insurance who had a dental visit in the past 12 months has increased from about 57% to 69%. However, for older adults who have some public dental insurance (mainly Medicaid) or who are uninsured, there has been no increase in dental services utilization in the past 20 years (Nasseh and Vujicic 2016; Yarbrough and Vujicic 2019).
Many older adults now receive a dental benefit through the purchase of a Medicare Advantage plan. Enrollment in these plans has increased from about 7% to 22%, with 2 out of 3 enrollees in these plans having a dental benefit (Jacobson et al. 2019). While the Patient Protection and Affordable Care Act of 2010 included dental care as an essential health benefit for children, it was not included for adults (Vujicic 2014). Medicare has never covered routine dental care, and the dental safety net for low-income adults remains limited, with only a few states offering comprehensive dental benefits to adults enrolled in Medicaid. Although the percentage of older adults with no dental insurance has declined from 64% to 57% over the past 2 decades, this age group continues to be the most likely not to have dental insurance compared to younger age groups, and older adults are the only age group that has seen an increase in out-of-pocket dental expenditures over the same period (See Section 1, Figure 13).
Studies have shown that a lack of dental insurance contributes to older adults having higher out-of-pocket expenses for dental care than other age groups. The mean out-of-pocket cost in 2015 for people who visited a dentist was $586 for retired adults 65 and older, compared with $264 for working adults and $220 for children and adolescents (Manksi and Rohde 2017). A lack of dental insurance is a major barrier to obtaining dental care and may account for the fact that 7.2% of older adults 65 and older—versus 4.3% of children—were more likely to report that they had forgone dental care in the past year because of cost (Vujicic et al. 2016). For more information on financing, see Section 4.
Another challenge for older adults is that they have more difficulty accessing dental care than younger adults or children because of physical and cognitive limitations. These limitations can make it difficult for them to maintain oral hygiene and withstand longer, complex dental procedures. Finally, lower perceived need for care is yet another barrier (Kiyak and Reichmuth 2005). Among adults with the same oral health status, those who are older consistently report lower perceived need for dental care than do younger adults (Griffin et al. 2012).
Provision of Older Adult Oral Health Care in Alternative Settings
Intergenerational and Family-Based Interventions
Progress over the past decade includes the development and implementation of intergenerational and family-based interventions for rural and immigrant communities that emphasize oral health promotion, disease prevention, and health literacy. These interventions include university-community partnerships, often employing community-based participatory research (CBPR) and qualitative approaches and methods (Huebner et al. 2014; Kavathe et al. 2018). Such interventions are based on the recognition that intergenerational influences—including caregivers’ attributes, attitudes, and knowledge—may contribute to the oral health of family members, along with societal and community influences, particularly in disadvantaged communities (Milgrom et al. 2013; Northridge et al. 2017a).
Community-Based Interventions
Since the last comprehensive report on oral health in 2000, CBPR approaches have been especially valuable in advancing community-based interventions designed to improve the oral health of American Indian/Alaska Native (AI/AN) populations in diverse settings (Cidro et al. 2014; Cidro et al. 2015; Cidro et al. 2017; Tiwari et al. 2018). Cidro and colleagues (2014) recommend that local health experts be included in discussions about health programs, including those for older adults, because opportunities to share traditions are essential to restoring skills and pride, building family and community relationships, and cultivating intergenerational support in Native communities. Moreover, it is essential for oral health professionals to understand the cultural health traditions of elders and their families to ensure community acceptance of the interventions (Cidro et al. 2015). Finally, community-based researchers should effectively communicate with members of these communities in culturally appropriate, nonjudgmental ways when discussing oral health behavior (Cidro et al. 2017). Together, these findings underscore that preferred methods for improving oral health in AI/AN communities include CBPR approaches, culturally tailored strategies, and joint implementation of the developed initiatives (Tiwari et al. 2018).
Discrimination makes it difficult for older adults, racial/ethnic minorities, and immigrants to obtain oral health prevention and treatment services (Lamster and Northridge 2008; Northridge et al. 2017b; Bastos et al. 2018; Hebert-Beirne et al. 2018). Focus groups conducted with racial/ethnic minority senior center attendees underscored the importance of respectful treatment in oral health programs and settings (Estrada et al. 2018). A CBPR study of Somali and Oromo refugees revealed the following health assets that may be used in culturally relevant health interventions: religious beliefs, religious and cultural practices, a strong culture of sharing, interconnectedness, the prominence of oral traditions, traditional healthy eating and healthy lifestyles, traditional foods and medicine, and a strong cultural value placed on health (Lightfoot et al. 2016). In-person, hands-on demonstrations of how to brush with fluoride toothpaste and floss properly using models, games, and other adult learning techniques delivered by trusted community educators in familiar settings were valued by Sikh-South Asian oral health promotion program participants (Northridge et al. 2017a).
Access to oral health care may be facilitated through community-based outreach activities with follow-up by patient navigators, program coordinators, and community health workers to ensure that adults and their families enroll in eligible dental insurance programs and link them to local dentists who accept their dental insurance (Northridge et al. 2017a; Widström et al. 2018) or to Federally Qualified Health Centers that provide dental care regardless of the ability to pay for services (Institute of Medicine and National Research Council 2011; Crall et al. 2016). Educational interventions designed through the CBPR approach for African American men in Atlanta (Hoffman et al. 2017) and functional, context-specific oral health literacy interventions developed and implemented by Indigenous staff in a rural location in South Australia (Ju et al. 2018) resulted in improved oral health literacy and related outcomes in these vulnerable adult populations.
Community-based oral health promotion interventions that combine oral health education with brief motivational interviewing, demonstrations of oral hygiene behaviors, and facilitated access to oral health care are underway for targeted groups of low-income, racial/ethnic minority adults and their families (Weinstein et al. 2014; Northridge et al. 2017a) and older adults (Marshall et al. 2013; Widström et al. 2018). The purpose of motivational interviewing is to create a discussion that engages the participant in thinking about and planning how to make positive behavior changes using such techniques as open-ended questions, reflective listening, and affirmations (Miller and Rollnick 2013; Weinstein et al. 2014).
Chapter 3. Promising New Directions
Advances in prevention and treatment, as well as the desire of individuals to keep their teeth as they age through adulthood, has reduced complete tooth loss and increased tooth retention to historical highs in the United States. The practical implications of this are that oral health providers will continue to provide fewer denture services and more preventive and restorative dental procedures aimed at preserving as many natural teeth as possible. Consequently, many promising new directions are focusing on improving access to care and care coordination.
Oral Health and General Health
The Oral Microbiome
One of the most important advances in biomedicine during the past 2 decades is a more thorough understanding of the oral microbiome, which is discussed in detail in Section 6. This new knowledge holds great promise for the future. The oral cavity, including its microbiome, is connected anatomically, immunologically, and metabolically to the rest of the body. Changes in the oral environment—particularly changes in oral pH levels induced by diet, oral hygiene, salivary flow, and the immune system—can cause a state of imbalance in the microbiome, characterized by an overgrowth of potentially harmful bacteria and changes in metabolic activity. This imbalance can cause oral diseases, such as dental caries and/or periodontal disease, and also may impact other aspects of human health, including diabetes.
Recently, saliva testing has received considerable attention as a noninvasive diagnostic tool for diabetes and for monitoring glucose in the blood. Salivary glucose levels are significantly associated with blood glucose and HbA1c levels in persons with type 1 (Naing and Mak 2017) and type 2 diabetes (Mascarenhas et al. 2014), especially at high levels of hyperglycemia. The combination of a panel of four salivary biomarkers with body mass index was able to accurately distinguish between high versus low insulin resistance among healthy and prediabetic individuals (Zhang et al. 2017). Several other salivary biomolecules have been associated with diabetes, supporting the potential value of saliva in the diagnosis and monitoring of diabetes (Zhang et al. 2016). However, more research is needed in salivary diagnostics, including the enrollment of study participants of advanced age who may have diminished salivary flow due to disease or medications and/or might benefit from less invasive testing procedures because of disability or frailty.
Osteoporosis Risk and Oral Health
Panoramic dental radiographs are widely used to support dental examinations. This technique has the potential to predict osteoporosis risk in older adults (Calciolari et al. 2015; Ohtsuki et al. 2017). One study showed that mandibular cortical width and the extent of erosion on panoramic radiographs were significantly correlated with bone mineral density, as measured using ultrasound densitometry, in older adults. Recent evidence suggests that panoramic radiography has much better utility at detecting osteopenia, rather than osteoporosis (Kinalski et al. 2020). Nevertheless, additional work is needed to verify this finding and advance this or other densitometry devices to the stage of widespread use for osteoporosis risk screening by oral health providers.
Medications and Polypharmacy
There are several new directions to advance the science and clinical management of people who take multiple medications, especially older adults. These include mechanistic-based research studies focused on bone and oral mucosal biology and looking for genetic markers for those who would be at risk for developing medication-related osteonecrosis of the jaw. Population health studies on antibiotic prophylaxis for infective endocarditis and prosthetic joint infection represent another promising area of research. The development of health professional curricula focused on interprofessional education and practice to improve care for older adults who may be under the care of multiple health professionals prescribing many medications is a strong area of need as well. Finally, dental professions could substantially advance the oral health of older adults through advocacy and involvement in pharmaceutical research, in particular for populations with limited representation in clinical trials, such as those with multiple medical conditions.
Prevention and Management of Oral Diseases and Conditions
Prevention and Management of Dental Caries
Most adults will experience some periodontitis as they age through adulthood, and this can result in some gingival recession and dental root exposure, which makes the tooth more vulnerable to dental caries on the root surface. There has been a resurgence in the use of silver diamine fluoride (SDF) to noninvasively treat root caries. Although further research is needed—especially longitudinal studies to assess long-term effectiveness in the elderly—it has been shown to be effective, affordable, and safe for use in older adults for this purpose (Crystal and Niederman 2019). SDF holds great promise to treat caries in homebound or institutionalized older adults because of ease of application and minimal support equipment needed to deliver this dental care service. The chemotherapeutic use of SDF may be an effective treatment for the management of other types of dental caries affecting older adults, and future use is expected to be adopted by a range of primary health care providers (Hendre et al. 2017).
Dental Caries Prevention in Cancer Survivors
Although home-applied fluorides for oral cancer patients going through radiation treatment have been studied, newer office-applied fluorides, such as fluoride varnish and SDF, have rarely been studied for their effectiveness as anticaries agents following cancer treatment (Gibson et al. 2011; Dholam et al. 2013; Chu et al. 2014; Jurasic et al. 2014; Hong et al. 2018). A novel product called casein phosphopeptide-amorphous calcium phosphate—a nanocomplex derived from milk protein usually used to manage incipient lesions but more recently used for irradiated patients—shows promise, but study populations have been small. Table 6 reviews several studies of calcium phosphate (Papas et al. 2008; Sim et al. 2015; Sim et al. 2019; Wu et al. 2019). Although these interventions are promising, more research is needed to provide oral health providers with sufficient evidence to guide clinical decision making.
Table 6
Studies using calcium phosphate in irradiated patients.
Special Needs Populations
Homebound Older Adults
Despite the challenges faced by homebound older adults, oral diseases in this population are preventable. Each member of the health care team who interacts with these vulnerable adults can promote the importance of toothbrushing, flossing, fluoride, nutrition, and diet (Critchlow 2017). Maintaining a healthy, functional dentition in homebound individuals is possible by using a collaborative, interprofessional approach to provide appropriate preventive measures and care and to address other barriers, such as minimal dental insurance, financial constraints, lack of perceived need, and functional dependency. Such individualized care can help prevent oral disease and maintain overall health, well-being, and quality of life (Yellowitz and Schneiderman 2014; Holm-Pedersen et al. 2015; Muller et al. 2017).
One example of collaboration involves meal delivery programs for homebound adults who have difficulty traveling to grocery stores or to senior centers for meals or who cannot cook because of mobility limitations or mental health problems. Recipients have had positive nutritional outcomes (Frongillo et al. 2010; Thomas and Dosa 2015). Using these interactions between the homebound and their meal deliverers as opportunities to discuss oral health would be a way to identify those who need oral health services and promote dental visits (Chamut et al. 2021).
Systems of Care for the Frail Elderly
The importance of oral health for older adults has caught the attention of those outside of dentistry who are working to improve systems of care for frail elders. For example, in 2017, the Gerontological Society of America proposed a variety of solutions for improving the oral health of older adults, including addressing barriers to access to dental care, identifying the need for interprofessional education and practice, promotion of an oral health benefit in Medicare, and creating coalitions and oral health champions for health promotion and public awareness campaigns while providing practical calls to action. An example of a current interprofessional solution is the MOTIVATE program (Maine’s Oral Team-Based Initiative: Vital Access to Education), established by Massachusetts General Hospital and the Lunder-Dineen Health Education Alliance of Maine. The program develops cross-disciplinary teams to provide oral health care to seniors living in long-term care facilities (Box 1).
In addition, the FDI/World Dental Federation has focused on oral health for an aging population by developing the Roadmap for Healthy Ageing, which calls for reinforcing prevention activities throughout the life course and adapting health systems to establish evidence-based prevention and care strategies (FDI World Dental Federation 2018). The following eight core pillars were identified: (1) integration of oral care into general care, (2) promotion of oral health throughout the life course, (3) shaping of evidence-based oral health policies, (4) removal of financial barriers, (5) removal of physical barriers, (6) provision of appropriate oral health care, (7) mobilization of all stakeholders along the care pathways, and (8) fostering of community-based programs. The Roadmap is a valuable resource as new systems of care focusing on prevention and dental-medical integration are developed and evaluated.
As previously mentioned, Seattle Care Pathways provides a patient-centered, evidence-based approach to care for well elders, as well as for others who are vulnerable. The FDI approach adds value, in that the FDI has applied the concepts of the Seattle Care Pathways for dental professionals, health care professionals, caregivers, community agencies, and seniors themselves with specific focus on what each group can contribute to improving oral health across the spectrum of dependency. The resultant interprofessional collaborative approach to care serves as an important resource for moving forward (FDI World Dental Federation 2018).
Dental Services Utilization
Since publication of the 2000 Surgeon General’s Report on Oral Health, more older adults have been able to access dental care through the purchase of a Medicare Advantage plan. Although this is an important mechanism for improving dental coverage for older adults, more than half of all older adults remain uninsured for dental services. More important, older adults are the only age group that has seen an increase in out-of-pocket dental expenditures during the last 2 decades (See Section 1 Figure 14).
Box 1How do communities train workers in long-term residential settings to improve the oral health care of seniors?
Because older adults who live in long-term care settings have unique risk factors and needs for oral health care, it is critical to provide them with evidence-based, routine oral health care. Organizations in Massachusetts and Maine collaborated to develop a program that provides interprofessional teams with education that advances knowledge, skills, and attitudes about the oral health needs of residents in long-term care. The MOTIVATE program (Maine’s Oral Team Based Initiative: Vital Access to Education) was established by the Lunder-Dineen Health Education Alliance of Maine, an initiative of Massachusetts General Hospital. A pilot program was implemented in 2016 in six homes in the Maine Veterans’ Home System that house 640 residents; more than 400 staff participated in the program. The Lunder-Dineen Health Education Alliance refined the program based on the pilot data, and the next phase involved expansion to a long-term care and rehabilitation system, increasing the number of involved residents to more than 900, and increasing participating staff to more than 700.
The curriculum for MOTIVATE targets a variety of staff: certified nursing assistants, dietary teams, facilities managers, housekeepers, nurses, pharmacists, social workers, and therapists (PT, OT, SLP, RT, ACT). These groups are trained to work as teams to provide oral health care, especially preventive services, for seniors. Every resident receives an oral health kit. The educational program includes online modules, live teaching sessions, and 6 months of onsite or virtual consultation. Online module topics include:
- Oral health leads to total health: Foundations of oral health care
- Tools of the trade: Steps in providing oral health care
- When to wait and when to act: Warning signs of oral health problems
- What to do when a resident has trouble with oral health care: Working together with residents and families
Partners include the University of New England College of Dental Medicine, University of Maine Center on Aging Research and Dental Hygiene Program, Maine Veterans’ Homes, Oral Health Progress and Equity Network (OPEN), Maine Dental Association, American Dental Association, CareQuest Institute for Oral Health, The Cedars, Island Nursing Home and Northern Light Health, and Mars Hill.
National and local policy and systems changes are important for creating communities that support good health and eliminating health inequities for older adults. Health policies can target a multitude of upstream social determinants of health, such as taxing sugary drinks, reducing carcinogenicity of meals provided in nursing homes, providing elder day care and home-delivered options for seniors, and increasing the availability of affordable fruits and vegetables in food deserts. At the same time, access to dental care, which also improves oral health, is essential. Older individuals who have the highest need are more likely than others not to have dental insurance (Oral Health America 2014; Kohli et al. 2017).
One of the most promising new directions that directly impacts improving oral health in older adults is the growing call for the inclusion of a dental benefit in Medicare, which provides universal medical coverage for adults 65 years and older. Inclusion of dental coverage in Medicare would be an important step toward addressing the complex factors that result in substantial inequities and hardship that many older adults experience trying to access oral health care. Other helpful initiatives include enhancing the oral health literacy of individuals and organizations and integrating medical and dental care, especially for medically compromised people with special needs from low-income and minority groups, including those in long-term care (Patrick et al. 2006). Nationally accepted guidelines for risk assessment and management are the standard of care for several aspects of elder medical care. The adoption of similar standards for frail older adults focusing on their oral health to ensure that they minimally have access to basic dental screenings, referrals, and preventive services would be a very important and promising step toward providing compassionate oral health care in later life.
Provision of Older Adult Oral Health Care in Alternative Settings
Interprofessional Care
Because many older Americans have difficulties with mobility and accessing dental care in a typical dentist’s office, options are now being explored using primary and interprofessional care. Many states already use venues such as congregate meal sites, assisted living facilities, and nursing homes to assess the oral health status of vulnerable older adults, using a simplified oral health screening tool from the Association of State and Territorial Dental Directors (Association of State and Territorial Dental Directors 2017). These programs can be expanded. Virtual dental homes also could increase access in dental shortage areas and among older adults who cannot easily visit a dental office. Teledentistry has been successful in providing virtual dental homes to adults of all ages (Glassman et al. 2012b). A study of nursing home residents found that remote dentists diagnosed dental pathologies with high accuracy (Queyroux et al. 2017).
Another promising direction is to promote the use of electronic health records, accountable care organizations, and coordinated care to better integrate oral health and medical care. Additional information on coordinated care is provided in Section 4. A 2011 Institute of Medicine report recommended that non-dental health care professionals take a more active role in the dental care of older adults living in long-term care facilities. The report found that with proper training, nurses, nursing assistants, and other health care workers could assess risk and screen for common oral conditions, educate residents about preventive oral care (such as daily brushing), and deliver preventive services, including daily oral hygiene care and fluoride varnish (Institute of Medicine and National Research Council 2011).
Comprehensive services using an interprofessional team may help reduce the prevalence of tooth loss for adults across age, racial/ethnic, and economic groups (Mertz and Wides 2016), which is a concern for older adults given the importance of a functional dentition and its relationship to overall well-being and quality of life. These services, including social and behavioral health services and diet/nutrition counseling, are needed to help prevent declines in nutrition status, poor health behaviors, and unhealthy dietary patterns that affect many older adults. To maximize the effectiveness of non-dental professionals in oral health roles, interprofessional education can teach them about the relationships between severe periodontitis and noncommunicable diseases, how to assess for periodontitis, and to make referrals to oral health care professionals for patients with poor oral hygiene or a suspected oral health problem.
Community-Based Interventions
Oral health equity for all adults will require embedding clear, culturally appropriate messages about the importance of oral health within community-based health interventions for other health concerns, such as tobacco prevention and cessation, improved nutrition, injury prevention, human papillomavirus vaccination, and diabetes prevention and control (Benzian and Williams 2015). Further, the broad reach of mobile technologies and digital lifestyles may provide opportunities for using remote monitoring and self-care tools to reinforce preventive oral hygiene behaviors that are critical to the maintenance of oral health (Shetty et al. 2018). Schensul and colleagues (2019) developed a protocol to implement a bilevel, community-based oral hygiene intervention among older adults and the disabled in low-income senior housing based on Fishbein’s Integrated Model of Behavior Change and Bandura’s concept of self-efficacy. The intervention consisted of a face-to-face tailored intervention based on adapted motivational interviewing and a building-based campaign developed and implemented by building residents. The campaign consisted of three oral health fairs. Six buildings were randomized to receive the individual-level intervention followed by the campaign. The cross-over research design addressed four questions: (1) Is the individual-based intervention more effective than the building-level intervention? (2) Does the sequence of the interventions matter? (3) What are the mechanisms that account for the differences? and (4) Are the improvements in outcomes sustainable? In addition to community-based participatory research and qualitative approaches, implementation science holds promise for addressing common barriers that limit the success of community-based oral health promotion (Simpson 2011).
Community Health Workers
A person’s culture can influence his or her health beliefs and behaviors, including those related to oral health. For relatively isolated older adult immigrants, community institutions and community health workers may serve as cultural brokers or bridges that link immigrants in the community to needed oral health information and resources (Marino et al. 2014; Kavathe et al. 2018). For example, low-cost, community-based peer support employing older adults/seniors designed to prevent diabetes also may improve oral health among underserved older adult populations (Thankappan et al. 2018).
Chapter 4. Summary
Too many older Americans experience poor oral health. They need and should receive better oral health care—integrated within the health care system—and better ways to access that care. As in younger populations, health inequities, in the forms of health disparities and limited and inconsistent access to care, persist and must be addressed. Overall, the prevalence of untreated decay in adults aged 65 and older has declined six percentage points since the year 2000, from approximately 28% to 22%. Unfortunately, untreated caries did not significantly decrease for older adults living in poverty (48% to 43%), whereas for more affluent older adults there was a significant decline (21% to 14%). Nearly 1 in 10 older adults has some form of severe periodontitis, with a much higher prevalence among men, lower-income seniors, and racial/ethnic minorities. Older adults continue to be the age group most often without dental insurance and with the highest out-of-pocket dental expenditures.
The older adult population in the United States is on course to outnumber the child/adolescent population (those 18 and younger) by 2034 (Vespa et al. 2018). By 2060, nearly 1 in 4 Americans (23.4%) will be 65 years or older. This burgeoning population puts pressure on a fragile oral health care infrastructure that has unequal distribution of services and prohibitive costs. Older adults at the highest risk for poor oral health tend to lack insurance and reside in underserved urban and rural areas, which also are factors shared by those who are economically disadvantaged and members of minority groups.
Resolving these inequities and barriers to care requires national legislation and other changes. Key actions are to add dental benefits to Medicare, to attract and retain skilled providers, to use evidenced-based care to achieve better outcomes, to offer adequate provider reimbursements, to establish nonemergency preventive and restorative dental services as an essential health component, and to support community-based oral health programs where older adults live and congregate. State and local legislative changes are needed to address transportation challenges, expand community outreach programs that increase health literacy, and boost oral health education. These initiatives have the potential to transform oral health care for older Americans.
Several key themes influencing older adult oral health have been described in this monograph (Box 2). Since the 2000 Surgeon General’s Report on oral health, new opportunities have emerged that focus on addressing shared risk factors and improving the management of noncommunicable diseases, improving interprofessional education and delivery of care, and identifying mechanisms to include oral health care as an integral part of our health care system. Specific gains in oral health over the last 20 years include a decrease in overall tooth loss, more research looking at periodontal disease as a source of chronic systemic inflammation, more clinical trials and analyses of treatment success for dry mouth, the identification of human papillomavirus as a risk factor for oropharyngeal cancer, and advances in the care of patients with oral cancer to decrease illness and death for those diagnosed at early stages. There also is better recognition of the potential impact of treatments for other types of cancers on oral health, more studies of systemic relationships between tooth loss and cognitive function and between the microbiome and diabetes mellitus, and new models for delivering dental care in nontraditional settings.
Many challenges to optimal oral health lie ahead for the rapidly increasing number of older adults in the United States, especially racial/ethnic minorities and those with lower incomes. Only 31% of older adults aged 65 to 74 and living in poverty have a functional dentition, compared to 74% of nonpoor older adults. Too many older adults face financial, logistical, and other barriers that keep them from improving and maintaining their oral health and accessing adequate oral health care.
Box 2Key summary messages for Oral Health Across the Lifespan: Older Adults
- Today, very few older adults lose all of their teeth as a result of improvements in disease prevention and treatment.
- Dental implants increasingly provide a safe and effective method for replacing lost teeth and for aiding in the retention of lower dentures; however, they remain a costly procedure and are out of the reach of most older adults.
- As working-age adults transition into retirement, most lose their employer-provided dental insurance, and Medicare does not provide an oral heath benefit. This puts their oral health at risk.
- Older adults are living longer than ever before, many with chronic diseases and complex health conditions that would be best managed by medical and oral health professionals working together.
- Older adults have a higher risk for poor oral health than any other age group because many of them lack dental insurance, have underlying health conditions, lack convenient access to care (especially those living in underserved urban and rural areas), and have limited financial resources. These factors result in the higher prevalence of many oral diseases in older adults, compared to younger adults.
- Receiving appropriate oral care can be especially difficult for older adults who are frail, disabled, homebound, cognitively impaired, or who reside in long-term care facilities. A coordinated team of caregivers is essential to address their care.
Call To Action:
- A policy that mandates dental coverage in Medicare would reduce health inequities for older adults by assuring access to preventive and other oral health services for all, including those who are place-bound or in need of caregiver assistance.
These difficulties are evident in the higher prevalence of many oral diseases in older adults than in younger adults. Systemic diseases and the medications used to treat them present specific and unique risks to oral health. For older adults who are disabled or homebound, achieving and receiving appropriate oral care can be a daily struggle.
Daunting and complex as they are, these challenges can be overcome. Targeted efforts in prevention and health literacy and novel approaches to make care more accessible and affordable are beginning to make inroads. Further, interprofessional approaches are emerging to better manage oral health within the broader health care system.
To be successful, however, barriers to oral health care must be more effectively addressed. Although older adults maintain more of their dentition into old age than ever before, many find themselves without the resources to afford dental care. Medicare, the primary form of health insurance for older Americans, specifically excludes dental services except in extremely limited circumstances. An estimated 70.8% of adults 65 and older had no dental insurance in 2017, and that percentage increases with age (Kramarow 2019). Removal of this exclusion and the inclusion of a universal and meaningful dental benefit available to all Medicare enrollees is essential for older adults to obtain needed care. This action would also establish oral health care as an essential element of health care systems.
For both researchers and clinicians, a better understanding of the underlying associations between oral diseases and medical diseases has revealed common risk factors and presented opportunities for treatment through interprofessional education and practice. A recent comprehensive review of systematic reviews has shown that additional research and evidence-based information are needed across most areas of geriatric oral health care, including in other disciplinary areas related to oral health (Ástvaldsdóttir et al. 2018). With the graying of America accelerating, this should be considered an urgent priority to improve the health and well-being of all Americans.
Integrated health teams that include dental providers will help eliminate oral health disparities and reduce health inequities among older adults. Too many older adults suffer disparities—in tooth loss, untreated decay, periodontal disease, and more—often related to social determinants of health, such as race/ethnicity and socioeconomic status. Using tooth loss as an example, the mean number of missing teeth decreased from about 14 to fewer than 11 missing teeth on average for non-Hispanic Blacks, whereas for non-Hispanic Whites, the decrease was nearly 9 to 6 missing teeth (Figure 15). For Mexican Americans, the decrease was from about 10 to 9 mean missing teeth. Even for older adults with the financial means to access dental care, there can be other barriers. Physical or cognitive disabilities, limited oral health literacy, and living in rural or underserved areas also present challenges in access to care, but none are insurmountable. Nontraditional models of care that focus on providing oral health promotion, prevention, and services in places where older adults live and gather show promise. Teledentistry and other innovations in oral care delivery are starting to make a difference, but additional resources and coordination are needed to expand their reach.
Our goal must be to ensure that older adults obtain appropriate oral health care, so that as they reach an advanced age or become frail or dependent, the primary focus can be on maintenance and prevention, rather than complex, invasive procedures that become a necessity after years or even decades of neglect. Achieving this goal will require improved access to care and maintenance of oral health for all older adults at all stages of health and dependency. Better oral health and oral health care for older Americans is achievable and critical to avoid new and recurrent oral diseases, to maintain dignity and quality of life, and to ensure general health and well-being through a lifetime.



